
Int. J. Front. Sci. , 8(1), 2; doi:10.37978/tijfs.v08i01.002
Review
Emerging Frontiers in Digital Health Transformation: Scope and Implementation Challenges in Low- and Middle-Income Countries—A Narrative Review
1
Independent Researcher, Witten, Germany
*
Correspondence: farzana.yasmin148@gmail.com
Academic Editor:
Muhammad Shoaib Akhtar
How to cite: Yasmin, F. Emerging Frontiers in Digital Health Transformation: Scope and Implementation Challenges in Low- and Middle-Income Countries—A Narrative Review. TIJFS 2026, 8 (1), 2. DOI: 10.37978/tijfs.v08i01.002.
Received: 13 February 2026 / Accepted: 11 June 2026 / Published: 1 July 2026
Abstract
:Background: Digital transformation has become essential for strengthening health systems in low- and middle-income countries (LMICs), which often experience workforce shortages, fragmented governance, inadequate infrastructure, and ongoing health inequities. Advances in artificial intelligence (AI), big data analytics, interoperability frameworks, precision medicine (PM), and connected health technologies present opportunities to improve access, quality, efficiency, and resilience within these systems. However, the implementation of these technologies remains inconsistent due to structural, regulatory, financial, and capacity-related barriers. This narrative review synthesizes current evidence on digital health transformation in LMICs, focusing on emerging technologies, system-level challenges, and future directions. Methods: A narrative literature review of peer-reviewed articles and grey literature published between 2015 and 2025 was conducted to examine digital health initiatives across health system functions. Results: LMICs have significant opportunities to utilize digital health to drive transformative reforms in their health systems. However, they face challenges stemming from a persistent “triple divide” that includes gaps in infrastructure, limitations in digital literacy, and disparities in data access. Additional barriers to progress include fragmented, non-interoperable systems; weak regulatory frameworks; deficiencies in data governance; infrastructure limitations; workforce shortages; algorithmic bias; and unequal access to resources. Promising solutions highlight the importance of developing interoperable digital public infrastructure (DPI), utilizing AI-enabled data harmonization, implementing federated learning, adapting governance models, and designing people-centered systems. Conclusions: Digital health has the potential to significantly enhance the resilience, equity, and sustainability of health systems in LMICs. This transformation can be achieved through coordinated national strategies, strong governance, inclusive and interoperable digital architectures, and consistent investment in workforce and institutional capacity. Future initiatives should prioritize ethical, context-sensitive AI, interoperability, and locally driven innovation to ensure lasting improvements in population health.
Keywords:
artificial intelligence; big data analytics; digital health; digital transformation; health system strengthening; Internet of Medical Things; interoperable health information systems; low- and middle-income countries1. Introduction
The digital revolution has significantly transformed healthcare systems worldwide. This transformation involves using information and communications technologies (ICTs) to enhance health and improve services. [1,2]. Initially focused on mobile health (m-health) and electronic health (e-Health), this transformation has now expanded to include emerging fields such as AI, genomics, advanced computing, and big data analytics [3]. The technologies encompass a wide range of applications, such as mobile phones and apps, wearable devices, electronic health records (EHRs), remote monitoring sensors, virtual care, robotics, and virtual reality (VR) [3,4]. These tools are increasingly utilized throughout the continuum of care. This continuum begins with prevention and health promotion, and extends to improve clinical decision-making, treatment effectiveness, access to care, chronic disease management, and the promotion of person-centred care (PCC) [3,5,6]. Healthcare providers and professionals play a crucial role in this transformation, applying technological innovations to address challenges within the health system and deliver high-quality care [4,7].
Digital transformation in healthcare is driven by several factors, including rapid technological advancement, the growing demand for data-driven clinical decision-making, PCC, and the maturation of analytical methods such as machine learning (ML) [4,7]. These developments enable the secure collection, processing, exchange, and near-real-time analysis of large volumes of clinical and non-clinical data. This not only fosters a more comprehensive approach to PCC but also enhances service management and supports population-level planning in both resource-rich and resource-constrained country settings [7,8,9,10]. This transformation is particularly crucial for LMICs. According to the World Bank, countries are categorized into four economic groups: low-income, lower-middle-income, upper-middle-income, and high-income. This classification is based on Gross National Income (GNI) per capita in U.S. dollars, converted from local currency using the Atlas method. For the 2026 fiscal year, low-income countries are defined as those with a GNI per capita of $1135 or less; lower-middle-income countries are between $1136 and $4495; upper-middle-income countries are between $4496 and $13,935; and high-income countries are those with a GNI per capita of $13,935 or more [11]. Many LMICs experience persistent challenges in their health systems, including shortages of the skilled health workforce, limited infrastructure, fragmented service delivery, barriers to access, and affordability issues [12,13]. Advances in health technologies offer a pathway to address gaps in the health system. The widespread use of mobile phones and growing availability of internet connectivity have accelerated the adoption of digital tools, such as EHRs, AI-enabled clinical decision-support systems, wearable monitoring devices, and ML applications. These innovations present opportunities to tackle the challenges mentioned earlier and enhance coordinated service delivery [6,14]. When integrated within interoperable digital ecosystems, these applications can reduce medical errors, enhance continuity of care, and strengthen overall health system performance [4,15].
The World Health Organization (WHO) has emphasized the significance of digital health as a crucial element in reaching its “triple billion” goals, which aim to expand universal health coverage (UHC) [3]. In many LMICs, digital health initiatives have evolved from small-scale, donor-driven projects into more comprehensive national strategies, a transition that was accelerated by the COVID-19 pandemic [15]. However, many of these interventions remain context-specific and narrowly focused, making it challenging to address broader system-level issues effectively [16].
By the end of 2025, approximately 82% of the global population owned a mobile phone, with about 58% utilizing mobile internet services. However, ownership of mobile phones and access to the internet in LMICs remain significantly lower [17]. In low-income countries (LICs), around 50% to 60% of the population owns a mobile phone, and the adoption of mobile internet is often limited by the issues of affordability and accessibility [13,17,18,19,20,21]. These disparities contribute to ongoing digital divides that influence the adoption and effectiveness of digital health interventions.
Additionally, structural barriers hinder the large-scale adoption of digital transformation. These barriers include inadequate digital infrastructure, limited interoperability between systems, privacy and cybersecurity risks, and underdeveloped regulatory frameworks [13,19]. Moreover, insufficient digital literacy among health professionals, policymakers, and patients further restricts the effective adoption and usage of digital applications. Without deliberate inclusive design, digital health solutions may exacerbate existing disparities in income, gender, literacy, and geographic location [22,23]. As a result, digital health transformation in LMICs remains uneven, characterized by varying levels of effectiveness, limited scalability, and concerns about sustainability [8].
To effectively address these challenges, we need coordinated, inclusive, and equitable strategies. Collaboration among governments, academic institutions, the private sector, and civil society is essential for transforming technological innovation into sustainable improvements in the health system. Strengthening governance frameworks, investing in shared and interoperable data infrastructures, and promoting knowledge exchange across sectors can ensure that the digital transformation significantly advances health equity and contributes to UHC in LMICs [24]. The objective of this narrative review is to provide a comprehensive understanding of emerging trends, key challenges, and future opportunities in the digital health transformation within LMIC health systems.
2. Methodology
2.1. Narrative Review Approach
A narrative literature review was conducted to synthesize published studies and grey literature on digital health transformation, particularly its implementation in LMICs. The review included a diverse range of sources, such as studies with various designs, literature reviews, case studies, policy reports, conference papers, and publications from international healthcare organizations. During the initial search and evaluation, key themes and priorities were identified based on factors such as relevance, recency, and contribution to understanding digital health transformation in LMICs.
2.1.1. Information Sources
In December 2025, a search was conducted across several databases, including PubMed, Google Scholar, Cochrane Library, and Google Search. Specific terms, outlined in the Box 1, were systematically combined using Boolean operators to capture a comprehensive set of relevant literature, policy documents, and global health reports on digital health transformation in LMICs. Additionally, more publications were identified through citation chasing of the selected studies. Targeted hand-searching of the websites and the publications of international organizations—such as the WHO, the World Bank, the United Nations Children’s Fund (UNICEF), and the United Nations Development Programme (UNDP)—was also carried out to locate relevant strategic frameworks, policy documents, and technical reports for inclusion in this review.
Box 1. Specific terms used to conduct search across databases.
Digital health, health technologies, digital transformation, digitalization, health care, mHealth, telemedicine, artificial intelligence, digital health information systems, digital tools, disease surveillance, LMICs.
2.1.2. Inclusion Criteria
This narrative review includes studies and reports that met the following criteria: (a) Economic setting: The studies must have been conducted in or relevant to LMICs, as defined by the World Bank classification at the time of publication [11]. (b) Topic relevance: Publications should focus on digital health interventions, systems, or policies. This includes mHealth, telemedicine and telehealth, EHRs and health information systems (HISs), AI and data analytics in healthcare, digital tools for disease surveillance, service delivery, or health workforce support, ML, PM, AI-driven data analysis, big data analytics, and internet of medical things (IoMT). (c) Health system relevance: Studies must address health-system-level outcomes, such as access to care, quality of services, efficiency, equity, governance, workforce capacity, or health system resilience. This includes case studies, but excludes any disease-specific pilot projects. (d) Study type: Eligible studies include peer-reviewed original research articles, review articles (narrative, scoping, or systematic reviews), and policy-relevant grey literature from international organizations (e.g., WHO, World Bank, UNICEF, UNDP). (e) Time frame: Publications should be dated between January 2015 and December 2025 to reflect the contemporary evolution of digital health in LMICs. (f) Language: Publications must be available in English.
2.1.3. Exclusion Criteria
Studies were excluded from the review if they met any of the following criteria: (a) Economic setting: Studies conducted exclusively in high-income countries that do not explicitly discuss their relevance or applicability to LMICs. (b) Limited digital health relevance: Publications that primarily focus on general information and communication technologies without clear applications in healthcare. This category includes studies that describe digital tools without assessing their implementation, usage, or implications for health systems. (c) Clinical focus without health system relevance: Studies that concentrate narrowly on clinical efficacy or technical performance without addressing health system integration, implementation, policy relevance, or broader service delivery implications. (d) Non-scholarly sources: Opinion pieces, editorials, commentaries, or blog posts. (e) Time frame: Publications that were published before 2015. (f) Language: Publications that are not available in English.
The table below presents the study protocol, illustrating the literature identification, screening, selection, and synthesis process undertaken in this review (Table 1).

Table 1.
The study protocol and the literature selection process.
| Items | Specification |
|---|---|
| Search period | 1–31 December 2025. |
| Database | PUBMED, Google Scholar, Cochrane Library, Google Search, Organizational websites (e.g., WHO, World Bank, UNICEF, UNDP). |
| Search Terms | Digital health, health technologies, digital transformation, digitalization, telemedicine, artificial intelligence, machine learning, digital health information systems, digital tools, precision medicine, AI-driven data analysis, big data analytics, Internet of Medical Things, LMIC. |
| Time Frame | January 2015 to December 2025. |
| Inclusion and exclusion criteria | Inclusion: peer-reviewed original articles; reviews; case studies; and grey literature/reports from WHO, World Bank, UNICEF, UNDP; English; studies conducted in LMICs. |
| Exclusion: non-peer-reviewed articles; editorials; conference papers; non-English; studies not conducted in or not relevant to LMICs. | |
| Selection process | F.Y. performed the search and made the final decision regarding selection. |
2.1.4. Study Selection
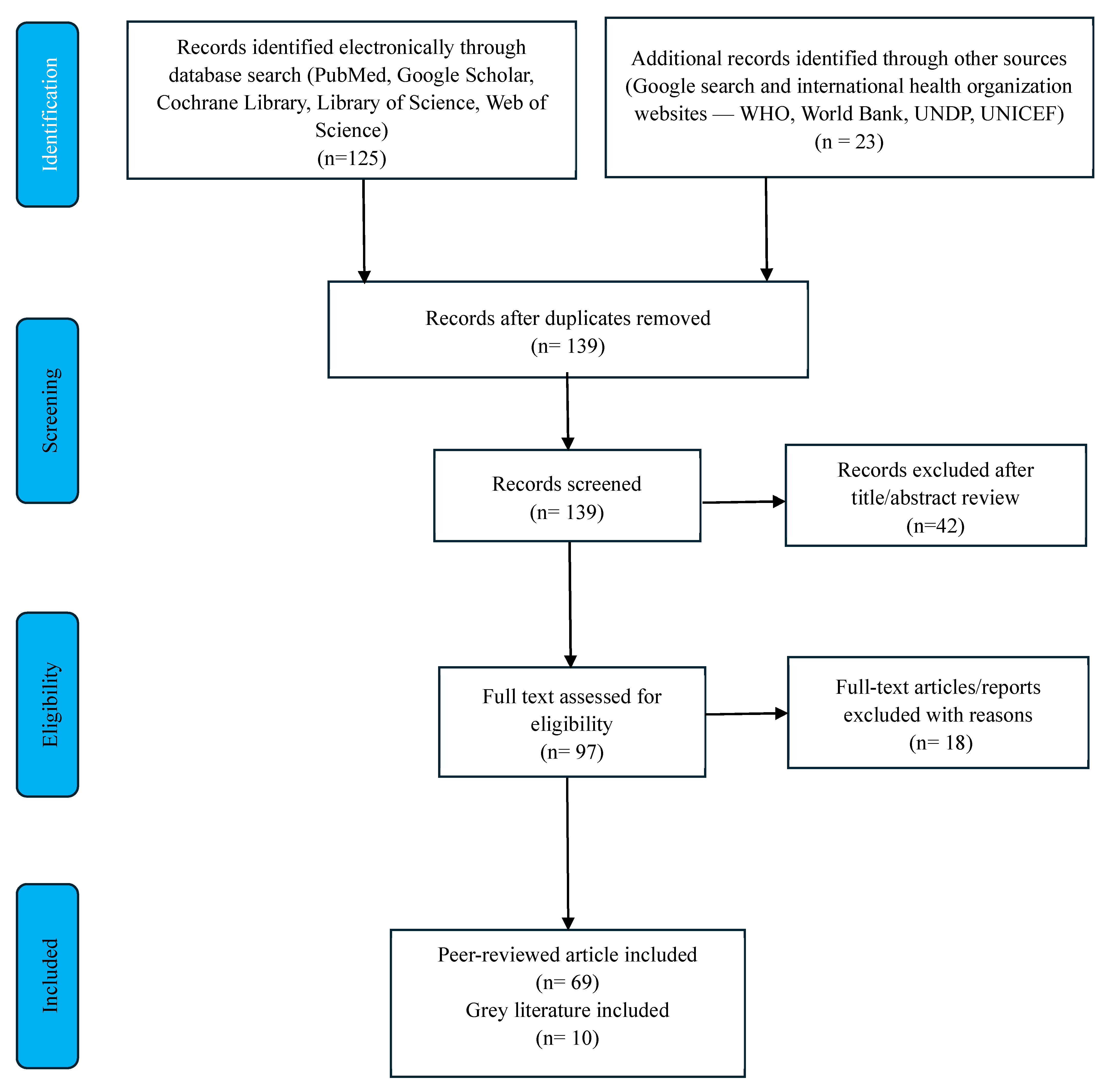
The author independently screened articles and grey literature identified during the initial search by reviewing their titles and abstracts. Publications that met the predefined inclusion criteria were selected for further assessment, while those that did not were excluded. The full texts of potentially relevant publications were then reviewed for final selection. The selection process was iterative, meaning that additional exclusions occurred during the synthesis and writing stages as thematic categories developed and relevance to the review objectives was reevaluated. Duplicate publications were identified and removed to prevent overlap in the synthesized evidence. A PRISMA flowchart was used to visualize the study selection process (Figure 1).
Figure 1.
Flow diagram of the literature search.
2.1.5. Data Extraction and Synthesis
Data extraction and synthesis were conducted using an iterative narrative review approach. A data extraction table was created to systematically organize relevant information from the included literature (see Supplement Document). This table included details such as title, authors, journal or organization name, publication type, and the primary focus of each study. Following data extraction, the findings were analysed using a manual inductive thematic coding approach. Initial codes were generated from the extracted data based on recurring concepts, patterns, and issues identified across the literature. These codes were reviewed and grouped into broader thematic categories through an iterative process of comparison and refinement.
The findings were subsequently synthesized through thematic narrative analysis. Studies were grouped based on recurring concepts, digital health domains, health system functions, implementation contexts, reported challenges, and proposed opportunities or future directions. Initial thematic categories were developed based on the frequency, relevance, and consistency of topics identified in the literature. Key themes included interoperability, AI, big data analytics, PM, IoMT, blockchain applications, governance and regulation, workforce capacity, and equity-related challenges.
To enhance the reliability of the thematic analysis, the emerging themes were cross-checked against the original publications throughout the synthesis process. Studies assigned to each theme were reviewed repeatedly to ensure consistency between extracted findings and the thematic categories. Themes were refined through iterative comparison across studies, and only themes supported by multiple publications were retained in the final synthesis. In addition, the identified themes were compared with existing global digital health frameworks, including the WHO digital health strategies and related policy guidance, to assess their conceptual consistency and relevance. Particular emphasis was placed on themes relevant across multiple LMIC contexts, reflecting broader sustainability and health system implications. The final thematic structure was refined iteratively to ensure coherence, conceptual clarity, and alignment with the review’s objectives.
3. Result
Over the past few decades, health systems worldwide have undergone significant digital transformation. In the 2010s, the focus was primarily on expanding mobile phone penetration and developing interactive mHealth applications [15,18]. The COVID-19 pandemic acted as a crucial catalyst, accelerating the adoption of telemedicine, digital surveillance systems, and virtual care models. These innovations enabled essential services to continue during the pandemic’s disruptive periods [25]. More recently, between 2024 and 2025, the rapid advancement of Generative AI and ML has emerged as a new frontier, providing innovative solutions to ongoing challenges within health systems [25].
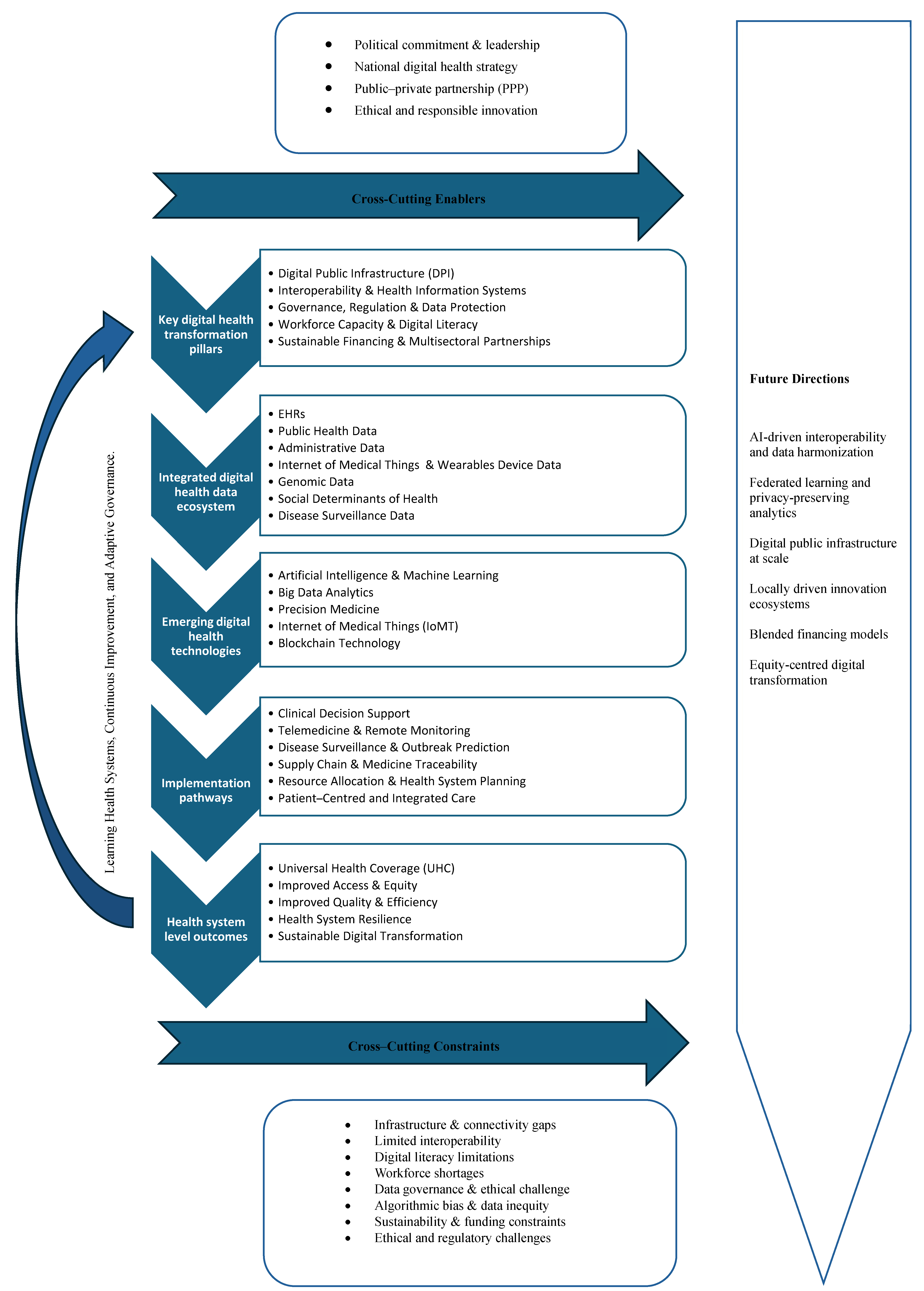
A conceptual framework has been developed to illustrate the relationships among the key pillars of digital health transformation, integrated health data ecosystems, emerging digital technologies, implementation pathways, and system-level outcomes (Figure 2). Cross-cutting constraints and enablers affect all stages of digital health transformation in LMICs.
Figure 2.
Conceptual framework of emerging digital health transformation in LMICs. The framework illustrates how foundational digital health pillars enable integrated data ecosystems that support emerging technologies, which are translated into practical health system applications and ultimately contribute to health system strengthening. Cross-cutting enablers and constraints influence implementation across all stages, while continuous learning and adaptive governance support long-term sustainability and improvement.
Figure 2.
Conceptual framework of emerging digital health transformation in LMICs. The framework illustrates how foundational digital health pillars enable integrated data ecosystems that support emerging technologies, which are translated into practical health system applications and ultimately contribute to health system strengthening. Cross-cutting enablers and constraints influence implementation across all stages, while continuous learning and adaptive governance support long-term sustainability and improvement.
This section provides a detailed overview of digital innovations in the health sector, exploring their specific applications and the outcomes they produce. The goal is to highlight how these technological advancements enhance healthcare delivery, improve patient outcomes, and transform traditional practices into more efficient and effective processes. This exploration will examine the advantages and challenges of implementing these innovations in real-world health settings, as well as their applications and outcomes. Notably, technologies such as PM, IoMT, and Blockchain may not be feasible to implement in LMICs in the near future.
3.1. Emerging Frontiers in Digital Health Transformation
3.1.1. Digital Health Data Integration Ecosystem—Interoperability
Interoperability is essential for digital healthcare systems [26,27]. EHRs play a vital role in improving health service delivery by centralizing patient information, improving data accessibility among providers, and enabling patients to access their own medical data [6,28,29]. Furthermore, integrating EHRs with biobanks and genomic databases has demonstrated significant potential to advance PM initiatives [26].
Digital Public Infrastructure
DPI provides a cohesive digital ecosystem that delivers services quickly and efficiently. When incorporated into the health system and coupled with AI-driven applications, DPI can serve as a catalyst for improving access, affordability, and quality of care. Interoperable data-sharing frameworks, digital identity systems, and real-time patient records enable AI algorithms to analyse extensive health data for purposes such as disease surveillance, early warning systems during public health emergencies, and PM applications. This integration has the potential to enhance patient outcomes and optimize resource allocation. According to the World Bank, DPI could advance UHC and facilitate the delivery of affordable, high-quality health services to up to 1.5 billion people by 2030. Additionally, AI-enhanced DPI improves supply chain transparency, medicine verification, and system resilience [30].
3.1.2. Integration of AI in Healthcare
AI-Driven Diagnostics and Generative AI
AI and ML have become critical tools for addressing challenges within health systems. These challenges include rising healthcare costs, the double burden of diseases, shortages of trained healthcare professionals, and inequities in access to healthcare services [31,32,33,34]. AI applications are increasingly transforming healthcare administration, service delivery, and public health infrastructure through methods such as ML, natural language processing, and systems for image and signal analysis [6,14,35,36]. Recently, large language models (LLMs) have been tested as decision-support “co-pilots” for community health workers, aiding in the translation of clinical guidelines into local languages and facilitating task delegation among healthcare providers. AI-driven analytics also support equity monitoring by identifying disparities in service utilization, thus informing policy responses. Furthermore, predictive analytics can enhance outbreak preparedness by enabling early detection and proactive resource allocation [34,37].
In LMICs, AI is being explored for various applications, including diagnostics, remote monitoring of chronic conditions, primary care delivery, disease surveillance, and outbreak prediction [3,6,25]. Given the significant workforce shortages in these regions, AI-enabled applications can serve as “force multipliers”, helping clinicians make faster decisions and allowing them to monitor more patients through remote tools. Automated triage systems can manage initial assessment, reducing the workload of primary care providers. Additionally, AI can help detect outbreaks earlier, thereby requiring fewer health professionals. These technologies enhance the effectiveness, reach, and productivity of existing healthcare workers and systems without necessitating a proportional increase in human resources [3,20,25,38].
AI-Driven Data Analysis
Secure and interoperable data exchange is crucial for both primary and secondary uses of health data. In primary contexts, it ensures continuity of care, enhances quality, and supports clinical decision-making. In secondary applications, it facilitates health systems research, population health analytics, and the validation, benchmarking, and deployment of AI and big data solutions [27]. In LMICs, AI-driven data analysis can significantly improve health system performance by addressing workforce shortages, overcoming fragmented HISs, and increasing access to specialist care. When integrated into an interoperable digital ecosystem, AI-enabled clinical applications can help standardize decision-making and extend the reach of limited specialist services [3,36].
By embedding AI within interoperable health systems, a variety of data sources, such as patient records, laboratory results, social determinants of health, administrative registries, and public health data, can be effectively integrated. This integration enhances continuity of care, supports clinical decision-making, improves system responsiveness, and aids in evidence-based policymaking [3,39,40]. Moreover, AI can facilitate the early detection of disease patterns and support healthcare workers, who are often overburdened, in delivering timely care. Predictive analytics can also facilitate more efficient allocation of scarce resources, such as staffing, diagnostics, and hospital capacity, ultimately strengthening overall health system efficiency. Additionally, when combined with interoperable HISs and DPI, this integration allows AI and ML models to function safely and contextually, supporting both clinical care and population-level decision-making [39,41].
3.1.3. Big Data Analytics in Healthcare
Big data analytics is crucial for transforming healthcare practices and research. It facilitates the acquisition, management, analysis, and integration of large volumes of diverse health data, both structured and unstructured [36]. This process leads to improved data-driven clinical decision support, optimized care delivery, and enhanced evidence-based health planning. Key areas of focus in this field include medical image processing, signal processing, and genomics [42]. High-dimensional imaging data are utilized to train deep learning models for diagnostics, risk assessment, and treatment planning. Additionally, continuous medical signals allow real-time monitoring, predictive analytics, and risk assessment. Advances in genomic sequencing further enhance AI-driven PM by enabling large-scale pattern recognition and risk stratification [36,42]. An example of effective implementation in Armenia is the development of a national cancer registry that incorporates genetic and genomic testing data. This registry is accessible to all clinics and laboratories nationwide and provides vital support for cancer patients. It is used for genetic testing and counselling for individuals with a high genetic predisposition and plays a role in PM initiatives [43]. By integrating various datasets into interoperable digital ecosystems, big data analytics empowers LMICs to implement predictive, personalized, and population-level interventions that address gaps in their health systems.
3.1.4. Precision Medicine
PM represents a significant shift in the prevention and treatment of diseases. It combines clinical, genetic, genomic, and epigenetic data to predict individual vulnerability, disease progression, and response to therapies [44,45,46,47]. Advances in AI and ML, along with interoperable data ecosystems, are essential for the successful implementation of PM [44]. By utilizing genomic sequencing and advanced analytics, clinicians can more accurately predict and tailor individualized treatment plans, reduce trial-and-error prescribing, and minimize adverse drug reactions [45,47,48]. In LMICs, PM offers considerable promise and substantial structural challenges. Key opportunities for PM in these regions include managing infectious and non-communicable diseases and applying pharmacogenomics [46,48,49].
Recently, there has been a shift toward “Precision Public Health,” which extends the principle of PM from focusing solely on individuals to implementing population-level interventions [39,50]. This approach uses integrated data on genomic and environmental factors, as well as social determinants of health, to enhance outbreak prediction, assess climate-related health risks, and guide targeted planning and resource allocation [39,50]. Considering that climate change disproportionately affects LMICs, it is vital to incorporate environmental and climate data into the digital ecosystem to improve preparedness and resilience [41]. However, to fully realize the potential of these innovations, we need strong data governance frameworks, ethical oversight, interoperable data ecosystems, and ongoing investment in local genomic, digital, and computational infrastructure, as well as the development of workforce capacity [38,39,46,50]. Meeting these requirements will pose a significant challenge for many LMICs in the foreseeable future.
3.1.5. The Internet of Medical Things and Remote Monitoring
The concept of a “hyperconnected healthcare ecosystem” has become a reality in many countries, including several middle-income countries (MICs). IoMT refers to the network of medical devices—such as wearables, implantable sensors, and smart hospital equipment—that provide real-time data [51]. By integrating these connected devices with an interoperable health ecosystem, IoMT facilitates a more responsive, data-driven approach to PCC. IoMT enables remote care in several ways, including: (a) testing and tracing for disease spread for infectious diseases, (b) real-time health monitoring, particularly for chronic disease management, (c) utilizing healthcare monitoring devices like smart pens, smart wearable devices like smart watches, smart implants, smart tooth brushes, sleep trackers, and loneliness detectors, (d) developing smart hospitals and smart operating rooms, (e) implementing smart medication-automated medication management, (f) tracing digital biomarkers, (g) providing robotic assistance, (h) supporting virtual planning and simulation- and navigation-guided surgery; (i) offering mobile and smartphone applications, (j) utilizing voice assistants; (k) enabling ambient assisted living; (l) detecting adverse drug reactions; and (m) facilitating telemedicine [51]. Furthermore, the integration of Metaverse technology into IoMT, through augmented reality (AR), mixed reality (MR), and VR offers opportunities for surgical training, rehabilitation, remote collaboration, and enhanced patient engagement [52,53,54,55].
3.1.6. Blockchain for Data Security and Supply Chain Integrity
Blockchain technology offers a promising solution for enhancing data security, patient-centred interoperability, and supply chain integrity within the digital health ecosystem [27]. By facilitating decentralized, secure digital data ledgers, blockchain has the potential to improve medical record management, streamline insurance claims processing, and support biomedical research [56,57]. This technology not only supports institution-driven interoperability models but also promotes a patient-centred interoperability approach, allowing individuals to access their own health information. This model is particularly relevant in LMICs, where internal migration is common, care pathways are often fragmented, and referral systems may be unreliable [27,56,58]. By shifting the control from institutions to individuals, blockchain-based systems could enhance transparency, trust, and accountability in health information exchange (HIE).
As digital health systems face an increasing threat of cyberattacks, blockchain provides enhanced protection of patient identity and data integrity through cryptographic validation and distributed consensus mechanisms [56]. Additionally, blockchain-based pharmaceutical traceability systems can help combat counterfeit medicines by tracking products throughout the supply chain, which is a critical concern in many LMICs [59,60].
4. Discussion
4.1. Key Challenges in Digital Health Transformation in LMICs
Despite rapid technological advancements and increased global investment, digital health transformation in LMICs continues to face persistent structural, systemic, and contextual challenges. Although the COVID-19 pandemic accelerated the adoption of digital applications, particularly telemedicine and digital surveillance, progress toward creating fully integrated and sustainable digital health ecosystems has been inconsistent. The challenges, often referred to as the “digital health divide,” can be categorized into four primary areas: infrastructure, literacy, governance, and equity. These factors hinder scalability, interoperability, and equitable health outcomes in many LMICs.
4.1.1. Infrastructure and Connectivity Gaps: The “Double Divide”
Inadequate digital infrastructure remains one of the most significant barriers to digital health transformation in LMICs. Many of these countries continue to struggle with unreliable power supplies, limited broadband coverage, and unstable internet connectivity. These issues hinder the advancement of HISs, cloud-based EHRs, and AI-enabled applications [27,61,62]. In addition to connectivity limitations, LMICs also experience a “hardware gap” across all levels of their health systems, which restricts the potential for digital transformation [25,62]. Although mobile phone penetration is relatively high in many LMICs, the quality, speed, and affordability of data services are often insufficient for supporting data-intensive applications, such as real-time remote monitoring or AI-driven decision-making [17,18].
Furthermore, disparities in infrastructure and access to services are widespread in most LMICs, exacerbating inequities in digital health adoption [16,63,64]. A shortage of skilled personnel is another critical barrier to progress [65]. If foundational infrastructure gaps are addressed, investments in AI, interoperable health ecosystems, and DPI risk deepening exist inequities, limiting scalability, and preventing digital health innovations from achieving the intended impact in LMIC health systems [18,64,65,66].
4.1.2. Digital Health Literacy and Workforce Capacity
The digital transformation in healthcare relies not only on the availability of digital infrastructure but also on workforce capacity and digital literacy of the workforce. A significant challenge identified in many LMICs is limited “digital readiness” [27,67]. Health workers often lack adequate training in digital applications, data interpretation, and AI-assisted decision-making, which diminishes the effectiveness and sustainability of digital health interventions. Additionally, there is a shortage of personnel with advanced technical and informatics skills, further hindering system maturity and preparedness for AI implementation [65]. Inadequate training in these areas leads to a lack of human resources, adversely impacting user safety and the overall effectiveness of health services [65].
Moreover, the outcomes of digital technologies can vary significantly among different population groups within a country or region [63]. Digital health initiatives risk exacerbating existing inequities by disproportionately benefiting individuals with higher levels of education or better digital skills. Patients with low literacy or limited experience using digital platforms may struggle to navigate applications or identify misinformation, which can ultimately erode trust in health systems [16,63].
4.1.3. Governance, Regulation, and Ethical Challenges
Data governance and regulatory frameworks pose significant barriers to digital health transformation in many LMICs. Many of these countries lack comprehensive policies regarding data protection, privacy, interoperability, and ethical oversight of digital health technologies [27,61,68]. Although consent mechanisms are often included in digital applications, users frequently lack awareness and understanding of the potential risks associated with the use or misuse of their data [68].
The integration of AI into healthcare has intensified these ethical and regulatory challenges. Key concerns include algorithmic bias, a lack of transparency in “black-box” models, data privacy and safety risks, and unclear liability for AI-driven clinical decisions [25]. Most LMICs lack a legal framework to govern AI accountability, particularly when models are trained on datasets from high-income countries that may not accurately reflect local populations and contexts. Weak governance further exacerbates these challenges, leading to inefficiencies, errors, waste, and corruption that undermine trust and compromise equitable service delivery [69,70]. As digital health initiatives evolve from pilot projects to national strategies, the absence of unified legal and governance frameworks has become a critical obstacle.
Robust governance frameworks are essential for the ethical and secure use of AI in digital health systems, particularly concerning patient data access and processing. Such frameworks may include strong safeguards for data privacy, cybersecurity, and informed consent, along with clear accountability for AI-driven decisions. Without these governance structures in place, the risk of misusing sensitive health data, experiencing algorithmic bias, and encountering opaque decision-making processes increases, disproportionately affecting vulnerable populations in LMICs [70]. Additionally, weak regulatory environments may exacerbate existing health inequalities if AI systems are trained on non-representative datasets or deployed without adequate validation in local contexts. These challenges can undermine public trust in digital health systems and hinder adoption by both healthcare providers and patients [69]. It is crucial to develop transparent regulatory standards, ethical guidelines, and context-sensitive governance mechanisms to ensure that AI contributes equitably and safely to strengthening health systems in LMIC settings [25,69,70].
4.1.4. Algorithmic Bias and Health Inequity
A growing concern in digital transformation in healthcare is the potential to unintentionally widen existing inequities. Algorithmic bias occurs when AI systems amplify disparities related to socioeconomic status, ethnicity, gender or sexual orientation, religion, disability, or geographic location. This poses significant challenges in many LMICs [27,65,71]. Disparities in access to technology raise important questions about equity [66]. AI models require large, high-quality, and representative datasets; however, LMIC populations are often underrepresented in these datasets. This underrepresentation leads to reduced accuracy and reliability for marginalized or low-income groups. Additionally, economic barriers, such as high costs for smart devices, internet connectivity, and data plans, create a “digital entry fee” that prevents nearly half of the LMIC populations from accessing digital health services. This situation undermines the goals of the WHO and the World Bank, which aim to advance digital transformation and achieve UHC [15]. Without a clear equity framework, digital health initiatives risk reinforcing the very disparities they seek to address.
4.1.5. Sustainability
Sustainability remains a critical challenge in digital health ecosystems in LMICs. Many initiatives in these settings are small-scale projects funded by donors that often lack clear pathways to scale up to the national level or to integrate into existing health systems. Various factors, such as reliance on external financing, high implementation costs, limited local technical expertise, corruption, and uncertain returns on investment, continue to hinder long-term viability [1,7,72]. To address these challenges, there is a fundamental shift toward sustainable and diversified financing models. Blended finance has emerged as a particularly promising approach, strategically combining public funding with private capital to mobilize private capital flows towards emerging and frontier markets, such as healthcare digitalization. By improving risk-adjusted returns, blended finance makes the digital health market more attractive to private investors and is increasingly utilized for public–private partnerships (PPPs) [73]. An example of a successful blended-finance model focused on healthcare innovation in Africa is Villgro Africa. It combines grant funding with impact investment, reducing risk for early-stage investors [74]. The open-source logistics management information system (LMIS) in Nigeria demonstrates a successful transition from donor-reliant models to private-sector stewardship through a PPP [74]. Multilateral development banks, such as the World Bank Group, the African Development Bank, and the Asian Development Bank, play a catalytic role in structuring and maximizing the use of these financial mechanisms. Additionally, the strategic alignment of Donor Investments in digital health is essential for coordinating fragmented funding around shared national priorities.
However, financial innovation alone is not sufficient. Achieving long-term sustainability requires leveraging local resources and strengthening multisectoral collaboration. Indonesia serves as a relevant example of effective multisectoral coordination in the development and national-scale implementation of digital health applications. This approach has enabled coordinated engagement across government ministries, the private sector, civil society, and development partners, demonstrating the achievements possible through coherent multisectoral governance [75].
Capacity-building is equally fundamental. Sustained investment in digital health competencies at the local level is crucial for the effective adoption, maintenance, and long-term sustainability of digital systems within local contexts. Without meaningful user engagement, adequate training, and seamless integration into clinical workflows, digital health interventions may face low uptake, user fatigue, and eventual abandonment. Overburdened healthcare providers often resist digital tools they perceive as adding to their administrative workload rather than improving service delivery. Thus, ensuring sustainability in digital health requires not only financial innovation but also institutional strengthening and workforce development to support long-term system integration [53].
4.2. Challenges in the Emerging Frontiers in Digital Health Transformation—Following the Themes
4.2.1. Short-Term Implementable Technologies
Digital Health Data Integration Ecosystem—Interoperability
Interoperability is essential for effective digital health ecosystems, especially as emerging technologies such as AI, blockchain, and federated learning become increasingly integrated into health systems [27,61]. However, in many LMICs, interoperability is often limited by fragmented digital landscapes. These landscapes are characterized by siloed information systems, incompatible platforms, and misaligned national policies [27,61]. Technical barriers are further complicated by legal fragmentation, weak institutional coordination, limited workforce capacity, and a lack of cohesive national digital health strategies [27].
Many HISs are designed to operate within provider- or institution-centric models that prioritize organizational workflows. Unfortunately, this approach restricts the sharing of longitudinal data, particularly in contexts where patients frequently move across facilities and regions [19,61]. From the perspective of PCC, there are additional gaps, including the limited integration of patient-generated health data (PGHD) into EHRs, a lack of user-friendly interfaces, and insufficient real-time feedback. These issues hinder patient engagement in care processes, compromising continuity of care, treatment adherence, service personalization, and the overall effectiveness of digital PCC strategies [26].
Integration of Artificial Intelligence in Healthcare
AI has the potential to significantly transform healthcare delivery and improve system efficiency. However, LMICs face numerous challenges in effectively adopting this technology. One major constraint is the quality and availability of data. AI models require large, representative, and continuously updated datasets. Unfortunately, many LMICs struggle with what is termed “data poverty,” where local populations are often underrepresented. This underrepresentation can lead to algorithmic bias and reduced accuracy in AI models [25,27,65,71]. Additionally, regulatory and ethical concerns impede implementation. Many LMICs lack comprehensive legal frameworks to ensure accountability in AI applications, transparency in the operation of “black-box” algorithms, and the protection of patient privacy [25,65,71]. Technical and infrastructure challenges also play a significant role. Issues such as limited computational capacity, unreliable internet connectivity, and restricted access to cloud-based resources hinder the scalable deployment of AI technologies [13,19]. Moreover, workforce gaps are a critical bottleneck. Shortages of trained data scientists, health informaticians, and clinicians skilled in AI integration compromise system readiness and long-term sustainability [8]. Lastly, issues of acceptability and trust persist. Both clinicians and patients may be hesitant to rely on AI-assisted decision-making because of unfamiliarity, perceived complexity, or concerns about errors and accountability [8,34]. To ensure that AI adoption is safe, equitable, and aligned with broader health-system-strengthening goals, it is essential to address these interconnected challenges.
Big Data Analytics in Healthcare
The effective implementation of big data analytics in LMICs faces several challenges. Data heterogeneity and quality: A significant concern is the quality and diversity of data. Clinical records, imaging, laboratory results, and administrative datasets are often incomplete, fragmented, or non-standardized. This compromises the reliability of analytic outputs and reduces the accuracy of AI-driven applications [42,51]. Infrastructure constraints: Many LMICs lack the high-performance computing capacity, secure cloud storage, and reliable network connectivity needed to process and manage large-scale datasets. The absence of Standards-Based Interoperability Infrastructure, such as Health Level Seven (HL7) Fast Healthcare Interoperability Resources (FHIR), limits the seamless integration of multi-source health data and undermines efforts to harmonize this information [25,33]. Workforce and skills gaps: There is a noticeable shortage of data scientists, bioinformaticians, and health professionals trained to interpret and operationalize analytical insights. This limits the ability to translate big data into actionable clinical and policy decisions [27,36,42]. These challenges significantly hinder the advancement of big data analytics in healthcare within LMICs. Additionally, privacy, ethical, and regulatory challenges persist. Protecting sensitive patient information, obtaining informed consent, and ensuring compliance with national and international regulations are particularly complex in resource-limited settings. Furthermore, when datasets are not representative, big data analytics may inadvertently reinforce existing inequities rather than promote equitable improvements in health systems [36,42,51].
4.2.2. Long-Term Prospective Technologies
Precision Medicine: Challenges in Genomic Data Integration
The implementation of PM in LMICs encounters significant challenges, particularly in integrating genomic data, safeguarding data privacy, ensuring regulatory compliance, and addressing limitations in computational capacity and infrastructure [44]. Infrastructure and Cost: Integrating large-scale genomic datasets with clinical and phenotypic information demands advanced computational infrastructure and secure data storage systems. When combined with AI-driven analytics, these requirements become technically complex and financially burdensome for many health systems [44,46]. Workforce Gap: The limited availability of trained professionals further hinders progress. Effective implementation of PM relies on bioinformaticians, genetic counsellors, molecular pathologists, and clinicians with expertise in genomics. However, such expertise is often scarce in many LMICs, and the inadequate incorporation of genomics into medical and health professional training programmes exacerbates this skills gap [42,72,76,77]. Data Inequity: Another significant barrier is the inequity in how data is represented. Global genomic research often disproportionately focuses on populations in high-income countries, particularly individuals of European ancestry [39]. This underrepresentation of LMIC populations in genomic databases restricts the validity, transferability, and equity of predictive models and precision tools across diverse genetic backgrounds [40,78,79]. Ethical and regulatory concerns: These issues complicate the adoption of PM. Concerns regarding informed consent, genetic discrimination, and the absence of harmonized cross-border data governance frameworks impede genomic data sharing. Compliance with international regulations, such as the Health Insurance Portability and Accountability Act (HIPAA) and the General Data Protection Regulation (GDPR), can be especially challenging in settings with limited legal and institutional capacity. Additionally, weak interoperability between genomic repositories and registries restricts the integration of genotype–phenotype relationships into routine clinical workflows. Overall, these structural, ethical, and technical constraints hinder the scalable, sustainable, and equitable implementation of PM in LMIC health systems [26,39,44,46,50,80].
The Internet of Medical Things and Remote Monitoring
The IoMT and remote patient monitoring systems hold significant potential for enhancing clinical care. However, their implementation in LMICs faces several technical, regulatory, and operational challenges. Data privacy and cybersecurity are primary concerns. IoMT systems continuously generate and transmit large volumes of sensitive health data across interconnected networks, making them susceptible to cyberattacks, unauthorized access, and data breaches [51,81]. Data management also presents additional challenges. Successful IoMT implementation requires robust mechanisms for data integration, synchronization, filtering, storage, and anonymization. These measures are essential to protect patient confidentiality while delivering clinically relevant information. The diversity of devices, proprietary platforms, and non-standardized data formats complicates seamless interoperability across systems. These issues are particularly pronounced in settings with limited bandwidth, unstable connectivity, and insufficient adherence to interoperability standards [51,81]. Scalability and system upgradability are crucial yet challenging in rapidly evolving technological landscapes. Continuous innovation demands frequent hardware replacements and software updates, which can be resource-intensive and unsustainable in low-resource settings [51,82]. Without long-term procurement and maintenance strategies, pilot deployments risk becoming fragmented and outdated. Cost-effectiveness represents another significant barrier. IoMT ecosystems rely on multiple sensors, wearable devices, connectivity infrastructure, and data management platforms, leading to substantial initial investment, ongoing maintenance, and replacement costs for both health systems and end users [50,75]. These financial burdens can restrict equitable access and long-term sustainability. Finally, power consumption and energy dependency remain ongoing limitations. Many IoMT devices rely on battery power, and frequent charging or replacement can be impractical in areas with unreliable electricity. The inefficiency of energy use, combined with limited access to stable power grids, hampers routine deployment and highlights the need for energy-efficient device design and integration with renewable energy solutions—an important consideration for many LMICs [51,82].
Blockchain for Data Security and Supply Chain Integrity
Implementing blockchain technology in health systems requires approaches that are safe, ethical, people-centred, cost-effective, and evidence-based [6,27]. Achieving these goals is particularly challenging in LMICs, where resource limitations, fragmented digital infrastructure, and context-specific operational barriers hinder adoption [56,58]. Many LMICs lack comprehensive national digital health strategies that explicitly assess and integrate blockchain solutions within broader health system priorities. Specifically, the absence of strategic planning hampers the careful evaluation of global blockchain-based platforms and shared digital services with respect to access, cost, quality, safety, and long-term sustainability [56,57].
4.3. Scope and Future Directions
Despite significant challenges, the evolving digital health landscape in LMICs presents substantial opportunities to improve health system design, governance, and service delivery. To leverage these opportunities, it is essential to move from fragmented, pilot-based initiatives to integrated, system-wide strategies for national digital transformation [6,18,62]. The following pillars are vital for successful and sustainable implementation.
4.3.1. Health System Strengthening and Resilience
Digital health has evolved from merely a collection of technological interventions to a foundational element for strengthening health systems in many LMICs. Its focus has expanded not only to improve service delivery but also to restructure the HIS, governance models, and frameworks for patient engagement.
Traditionally, many health systems in LMICs have relied on paper-based records, resulting in fragmented data flows, insufficient continuity of care, and limited evidence to inform planning and decision-making. The expansion of EHRs and interoperable digital platforms presents an opportunity to enable real-time data access, improve care coordination, and enhance system responsiveness and resilience, especially during public health emergencies [6,12,62]. For example, Angola has improved Tuberculosis (TB) surveillance through the Electronic Medical Record System (EMRS), resulting in better patient care [83]. In Rwanda, the introduction of a national HIE that uses a unique patient identifier has successfully ensured continuity of care across public and private facilities, marking a significant advancement in the country’s digital health transformation [84]. Similarly, Brazil has established a unified national health system to create a comprehensive database for epidemiological, administrative, and clinical purposes [85]. In addition to developing infrastructure, it is essential to enhance digital literacy and workforce capacity [62,72]. Building competencies in data management, digital applications, and AI-supported decision-making is critical for ensuring the effective adoption and long-term sustainability of digital transformation initiatives [6,18,72]. Lastly, policy alignment and governance are vital for supporting these advancements.
4.3.2. Policy Alignment and Governance Frameworks
A critical future direction for digital health transformation in LMICs is to align policies and strengthen governance mechanisms. As digital health ecosystems become more complex, data-driven, and interconnected, establishing coherent regulatory and institutional frameworks becomes essential. These frameworks are crucial for protecting data privacy, ensuring ethical deployment of AI, strengthening cybersecurity, and enabling secure cross-border data exchange [27,61,70]. Global coordination platforms, such as the Global Initiative on Digital Health (GIDH), provide valuable opportunities to harmonize standards, promote interoperability, facilitate knowledge exchange, and support countries in developing context-specific digital health roadmaps [86]. Strengthening the alignment between global frameworks and national implementation strategies will be vital for ensuring that digital transformation efforts are scalable, secure, and equitable.
4.3.3. Local Innovation and Public–Private Partnerships
An important future direction for HISs is the transition to “loose coupling” architectures. Unlike rigid, monolithic platforms, loosely coupled systems enable modular design, enabling various applications to work together through shared standards and open interfaces. This approach enhances flexibility, scalability, and adaptability—qualities that are especially critical in LMICs, which often face resource constraints and rapidly changing health priorities [15]. Promoting local innovation within interoperable ecosystems allows governments, startups, academic institutions, and private-sector entities to develop digital solutions tailored to local needs. A prime example is the Rwanda Health Information Exchange (RHIE), an interoperability framework that facilitates communication and data exchange across healthcare systems. By integrating healthcare data in accordance with global standards, RHIE has improved data accuracy, accessibility, and real-time sharing of patient information, including visit summaries, diagnostic results, and treatment histories. This integration supports continuity of care and informed clinical decision-making [84].
PPPs can further accelerate innovation, expand technical expertise, and mobilize investment that aligns with national health strategies and public interest objectives [15]. Rwanda’s focus on engaging the private and academic sectors through PPPs has been crucial to its success in transforming healthcare through digital solutions. These partnerships ensure that the health workforce becomes digitally literate and is prepared to utilize the technology integrated into Rwanda’s health systems [84].
4.3.4. Scalable, Interoperable, and People-Centred Digital Solutions
The future of digital health revolves around moving away from isolated, pilot-based initiatives and transitioning toward integrated national digital ecosystems aligned with UHC goals. A noteworthy example of this is Indonesia, which successfully implemented a national-scale digital management system in response to the COVID-19 pandemic. This system encompassed detection, prevention, treatment, and monitoring [75]. Resilient health systems will increasingly depend on interoperable, scalable, and people-centred DPI to enhance service delivery. This approach closely aligns with the core objectives of the WHO Global Strategy on Digital Health, which emphasizes global collaboration, strong governance, and systems that prioritize people, all empowered by digital technologies [6,27,61,72].
4.4. Limitations
This study is a narrative review, which means it does not provide a systematic evaluation of all available evidence. The findings may be influenced by publication bias, selective reporting, and differences in study quality. Additionally, the review may not fully include regional reports or other grey literature that could offer important contextual insights. The diversity of study designs, health system contexts, and digital health interventions also limits the generalizability of the conclusions. Despite these limitations, this review offers a thorough synthesis of key themes and emerging issues important to the transformation of digital health in LMICs.
5. Conclusions
LMICs have a unique opportunity to leverage digital health as a catalyst for transformative change within their health systems. This review highlights that achieving sustainable digital health transformation requires strategic alignment with national health priorities, strong governance frameworks, interoperable systems, and ongoing investment in workforce capacity. Emerging technologies, such as AI and advanced analytics, have significant potential to enhance efficiency, improve clinical decision-making, and support population health. However, their implementation must prioritize fairness, transparency, and contextual relevance to avoid perpetuating existing inequities.
An approach that emphasizes equity, is centred on people, and is supported by inclusive design, robust data governance, and locally driven innovation is crucial to ensuring that digital health provides meaningful benefits to underserved populations. By integrating digital health within broader health systems and policy reforms, and by moving beyond fragmented pilot initiatives to establish a cohesive DPI, LMICs can accelerate progress toward UHC and improve health outcomes for their populations.
Supplementary Materials
The following supporting information can be downloaded at: https://tijfs.jams.pub/.
Funding
This research received no external funding.
Data Availability Statement
All information analyzed in this study was obtained from publicly available published sources cited in the reference list. No new datasets were generated.
Acknowledgments
ChatGPT 5.2 and Grammarly were used to proofread and improve grammar.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Kostkova, P. Grand challenges in digital health. Front. Public Health 2015, 3, 134. [Google Scholar] [CrossRef] [PubMed]
- Belliger, A.; Krieger, D.J. The digital transformation of healthcare. In Knowledge Management in Digital Change: New Findings and Practical Cases; Springer International Publishing: Cham, Switzerland, 2018; pp. 311–326. [Google Scholar]
- WHO. Recommendations on Digital Interventions for Health System Strengthening; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ahmed, M.M.; Okesanya, O.J.; Olaleke, N.O.; Adigun, O.A.; Adebayo, U.O.; Oso, T.A.; Eshun, G.; Lucero-Prisno, D.E. Integrating Digital Health Innovations to Achieve Universal Health Coverage: Promoting Health Outcomes and Quality Through Global Public Health Equity. Healthcare 2025, 13, 1060. [Google Scholar] [CrossRef] [PubMed]
- Bhavnani, S.P.; Narula, J.; Sengupta, P.P. Mobile technology and the digitization of healthcare. Eur. Heart J. 2016, 37, 1428–1438. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Strategy on Digital Health 2020–2027; WHO (World Health Organization): Geneva, Switzerland, 2025. [Google Scholar]
- Craig, A.; Lawford, H.; Miller, M.; Chen-Cao, L.; Woods, L.; Liaw, S.T.; Godinho, M.A. Use of Technology to Support Health Care Providers Delivering Care in Low- and Lower-Middle-Income Countries: Systematic Umbrella Review. J. Med. Internet Res. 2025, 27, e66288. [Google Scholar] [CrossRef] [PubMed]
- Stoumpos, A.I.; Kitsios, F.; Talias, M.A. Digital Transformation in Healthcare: Technology Acceptance and Its Applications. Int. J. Environ. Res. Public Health 2023, 20, 3407. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, E. Healthcare and digital transformation. Netw. Secur. 2017, 2017, 7–11. [Google Scholar] [CrossRef]
- Kraus, S.; Schiavone, F.; Pluzhnikova, A.; Invernizzi, A.C. Digital transformation in healthcare: Analyzing the current state-of research. J. Bus. Res. 2021, 123, 557–567. [Google Scholar] [CrossRef]
- Bank, T.W. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 11 May 2026).
- Bae, J.; Bhatt, A. Building Stronger Health Care Systems: Digital Health’s Vital Role in Empowering the LMIC Health Workforce. JACC Adv. 2024, 3, 100953. [Google Scholar] [CrossRef] [PubMed]
- Yao, R.; Zhang, W.; Evans, R.; Cao, G.; Rui, T.; Shen, L. Inequities in Health Care Services Caused by the Adoption of Digital Health Technologies: Scoping Review. J. Med. Internet Res. 2022, 24, e34144. [Google Scholar] [CrossRef] [PubMed]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Future Healthc. J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Sylla, B.; Ismaila, O.; Diallo, G. 25 Years of Digital Health Toward Universal Health Coverage in Low- and Middle-Income Countries: Rapid Systematic Review. J. Med. Internet Res. 2025, 27, e59042. [Google Scholar] [CrossRef] [PubMed]
- McCool, J.; Dobson, R.; Whittaker, R.; Paton, C. Mobile Health (mHealth) in Low- and Middle-Income Countries. Annu. Rev. Public Health 2022, 43, 525–539. [Google Scholar] [CrossRef] [PubMed]
- ITU (International Telecommunication Union). Global Connectivity Report 2025. Assessing Progress toward Universal and Meaningful Connectivity; International Telecommunication Union: Geneva, Switzerland, 2026. [Google Scholar]
- Onigbogi, O.; Ojo, O.Y.; Kinnunen, U.M.; Saranto, K. Mobile health interventions on vaccination coverage among children under 5 years of age in Low and Middle-Income countries; a scoping review. Front. Public Health 2025, 13, 1392709. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.; Yam, E.L.Y.; Cheruvettolil, K.; Linos, E.; Gupta, A.; Palaniappan, L.; Rajeshuni, N.; Vaska, K.G.; Schulman, K.; Eggleston, K.N. Perspectives of Digital Health Innovations in Low- and Middle-Income Health Care Systems From South and Southeast Asia. J. Med. Internet Res. 2024, 26, e57612. [Google Scholar] [CrossRef] [PubMed]
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [PubMed]
- Latulippe, K.; Hamel, C.; Giroux, D. Social Health Inequalities and eHealth: A Literature Review With Qualitative Synthesis of Theoretical and Empirical Studies. J. Med. Internet Res. 2017, 19, e136. [Google Scholar] [CrossRef] [PubMed]
- Makri, A. Bridging the digital divide in health care. Lancet Digit. Health 2019, 1, e204–e205. [Google Scholar] [CrossRef]
- Yu, J.; Meng, S. Impacts of the Internet on Health Inequality and Healthcare Access: A Cross-Country Study. Front. Public Health 2022, 10, 935608. [Google Scholar] [CrossRef] [PubMed]
- van de Vijver, S.; Tensen, P.; Asiki, G.; Requena-Mendez, A.; Heidenrijk, M.; Stronks, K.; Cobelens, F.; Bont, J.; Agyemang, C. Digital health for all: How digital health could reduce inequality and increase universal health coverage. Digit. Health 2023, 9, 20552076231185434. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.; Barcellona, C.; Mandyam, N.K.; Tan, S.Y.; Tromp, J. Challenges and Opportunities for Data Sharing Related to Artificial Intelligence Tools in Health Care in Low- and Middle-Income Countries: Systematic Review and Case Study From Thailand. J. Med. Internet Res. 2025, 27, e58338. [Google Scholar] [CrossRef] [PubMed]
- Ambalavanan, R.; Snead, R.S.; Marczika, J.; Towett, G.; Malioukis, A.; Mbogori-Kairichi, M. Challenges and strategies in building a foundational digital health data integration ecosystem: A systematic review and thematic synthesis. Front. Health Serv. 2025, 5, 1600689. [Google Scholar] [CrossRef] [PubMed]
- Adegoke, K.; Adegoke, A.; Dawodu, D.; Adekoya, A.; Bayowa, A.; Kayode, T.; Singh, M. Interoperability as a Catalyst for Digital Health and Therapeutics: A Scoping Review of Emerging Technologies and Standards (2015–2025). Int. J. Environ. Res. Public Health 2025, 22, 1535. [Google Scholar] [CrossRef] [PubMed]
- Pawelek, J.; Baca-Motes, K.; Pandit, J.A.; Berk, B.B.; Ramos, E. The Power of Patient Engagement With Electronic Health Records as Research Participants. JMIR Med. Inf. 2022, 10, e39145. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb. Med. Inf. 2016, 25 (Suppl. 1), S48–S61. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.; Marin, G.; Ardic Alper, O.P.; Galicia Rabadan, G.A. Digital Public Infrastructure and Development: A World Bank Group Approach. Digital Transformation White Paper; The World Bank: Washington, DC, USA, 2025; Volume 1. [Google Scholar]
- Xu, Y.; Liu, X.; Cao, X.; Huang, C.; Liu, E.; Qian, S.; Liu, X.; Wu, Y.; Dong, F.; Qiu, C.W.; et al. Artificial intelligence: A powerful paradigm for scientific research. Innovation 2021, 2, 100179. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Pandit, A.; Shukla, S. Transforming healthcare with big data analytics and artificial intelligence: A systematic mapping study. J. Biomed. Inf. 2019, 100, 103311. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Ngiam, K.Y.; Teo, H.H. Role of Artificial Intelligence Applications in Real-Life Clinical Practice: Systematic Review. J. Med. Internet Res. 2021, 23, e25759. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Saiso, S.; Marti, M.; Pesce, K.; Luciani, S.; Mujica, O.; Hennis, A.; D’Agostino, M. Artificial Intelligence as a Potential Catalyst to a More Equitable Cancer Care. JMIR Cancer 2024, 10, e57276. [Google Scholar] [CrossRef] [PubMed]
- Aung, Y.Y.M.; Wong, D.C.S.; Ting, D.S.W. The promise of artificial intelligence: A review of the opportunities and challenges of artificial intelligence in healthcare. Br. Med. Bull. 2021, 139, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Ciecierski-Holmes, T.; Singh, R.; Axt, M.; Brenner, S.; Barteit, S. Artificial intelligence for strengthening healthcare systems in low- and middle-income countries: A systematic scoping review. npj Digit. Med. 2022, 5, 162. [Google Scholar] [CrossRef] [PubMed]
- Sendak, M.; Balu, S.; Hernandez, A.F. Proactive Algorithm Monitoring to Ensure Health Equity. JAMA Netw. Open 2023, 6, e2345022. [Google Scholar] [CrossRef] [PubMed]
- Holmer, H.; Lantz, A.; Kunjumen, T.; Finlayson, S.; Hoyler, M.; Siyam, A.; Montenegro, H.; Kelley, E.T.; Campbell, J.; Cherian, M.N.; et al. Global distribution of surgeons, anaesthesiologists, and obstetricians. Lancet Glob. Health 2015, 3 (Suppl. 2), S9–S11. [Google Scholar] [CrossRef] [PubMed]
- Rebecca, B.; Annette, B.; Emma, F.; Carter, S. The emergence and future of precision public health: A scoping review. Health Policy Technol. 2025, 14(5), 101056. [Google Scholar] [CrossRef]
- Misra, S.; Aguilar-Salinas, C.A.; Chikowore, T.; Konradsen, F.; Ma, R.C.W.; Mbau, L.; Mohan, V.; Morton, R.W.; Nyirenda, M.J.; Tapela, N.; et al. The case for precision medicine in the prevention, diagnosis, and treatment of cardiometabolic diseases in low-income and middle-income countries. Lancet Diabetes Endocrinol. 2023, 11, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.G. Using Precision Public Health to Manage Climate Change: Opportunities, Challenges, and Health Justice. J. Law Med. Ethics 2021, 48, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Belle, A.; Thiagarajan, R.; Soroushmehr, S.M.; Navidi, F.; Beard, D.A.; Najarian, K. Big Data Analytics in Healthcare. Biomed. Res. Int. 2015, 2015, 370194. [Google Scholar] [CrossRef] [PubMed]
- Babikyan, D.; Sarkisian, T. Digitization in Genetics and Diagnostics Laboratories in Armenia. In Digitalization of Medicine in Low- and Middle-Income Countries; Kozlakidis, Z., Muradyan, A., Sargsyan, K., Eds.; Springer: Cham, Switzerland, 2024. [Google Scholar]
- Akhoon, N. Precision Medicine: A New Paradigm in Therapeutics. Int. J. Prev. Med. 2021, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Chow, N.; Gallo, L.; Busse, J.W. Evidence-based medicine and precision medicine: Complementary approaches to clinical decision-making. Precis. Clin. Med. 2018, 1, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Anaya, J.M.; Herrán, M.; Pino, L.E. Challenges and opportunities for precision medicine in developing nations. Expert. Rev. Precis. Med. Drug Dev. 2025, 10, 1–15. [Google Scholar] [CrossRef]
- Peck, R.W. Precision Medicine Is Not Just Genomics: The Right Dose for Every Patient. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Dugger, S.A.; Platt, A.; Goldstein, D.B. Drug development in the era of precision medicine. Nat. Rev. Drug Discov. 2018, 17, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Zgheib, N.K.; Patrinos, G.P.; Akika, R.; Mahfouz, R. Precision Medicine in Low- and Middle-Income Countries. Clin. Pharmacol. Ther. 2020, 107, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Canfell, O.J.; Davidson, K.; Woods, L.; Sullivan, C.; Cocoros, N.M.; Klompas, M.; Zambarano, B.; Eakin, E.; Littlewood, R.; Burton-Jones, A. Precision Public Health for Non-communicable Diseases: An Emerging Strategic Roadmap and Multinational Use Cases. Front. Public Health 2022, 10, 854525. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, R.; Mehrotra, D.; Chandra, S. Potential of Internet of Medical Things (IoMT) applications in building a smart healthcare system: A systematic review. J. Oral Biol. Craniofac. Res. 2022, 12, 302–318. [Google Scholar] [CrossRef] [PubMed]
- Kye, B.; Han, N.; Kim, E.; Park, Y.; Jo, S. Educational applications of metaverse: Possibilities and limitations. J. Educ. Eval. Health Prof. 2021, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Yew, S.Q.; Trivedi, D.; Adanan, N.I.H.; Chew, B.H. Facilitators and Barriers to the Implementation of Digital Health Technologies in Hospital Settings in Lower- and Middle-Income Countries Since the Onset of the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2025, 27, e63482. [Google Scholar] [CrossRef] [PubMed]
- Petrigna, L.; Musumeci, G. The Metaverse: A New Challenge for the Healthcare System: A Scoping Review. J. Funct. Morphol. Kinesiol. 2022, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Eckert, M.; Volmerg, J.S.; Friedrich, C.M. Augmented Reality in Medicine: Systematic and Bibliographic Review. JMIR Mhealth Uhealth 2019, 7, e10967. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J. Blockchain Technology and Healthcare. Healthc. Inf. Res. 2019, 25, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Kuo, T.T.; Kim, H.E.; Ohno-Machado, L. Blockchain distributed ledger technologies for biomedical and health care applications. J. Am. Med. Inf. Assoc. 2017, 24, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Gordon, W.J.; Catalini, C. Blockchain Technology for Healthcare: Facilitating the Transition to Patient-Driven Interoperability. Comput. Struct. Biotechnol. J. 2018, 16, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Mani, V.; Prakash, M.; Lai, W.C. Cloud-based blockchain technology to identify counterfeits. J. Cloud Comput. 2022, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Islam, I.; Islam, M.N. A blockchain based medicine production and distribution framework to prevent medicine counterfeit. J. King Saud. Univ.—Comput. Inf. Sci. 2024, 36(3–4), 101851. [Google Scholar] [CrossRef]
- Jayathissa, P.T.; Hewapathirana, R. Enhancing Interoperability among Health Information Systems in Low and Middle- Income Countries: A Review of Challenges and Strategies. Eur. Mod. Stud. J. 2023, 7, 334–340. [Google Scholar] [CrossRef]
- UNDP. Enhancing Digital Transformation in the Health Sector in Vietnam. A Case Study on Application of Electronic Health Records in Lang Son, Binh Thuan and Tay Ninh Provinces; UNDP (Ireland): Dublin, Ireland, 2024. [Google Scholar]
- Western, M.J.; Smit, E.S.; Gultzow, T.; Neter, E.; Sniehotta, F.F.; Malkowski, O.S.; Wright, C.; Busse, H.; Peuters, C.; Rehackova, L.; et al. Bridging the digital health divide: A narrative review of the causes, implications, and solutions for digital health inequalities. Health Psychol. Behav. Med. 2025, 13, 2493139. [Google Scholar] [CrossRef] [PubMed]
- Monlezun, D.J.; Omutoko, L.; Oduor, P.; Kokonya, D.; Rayel, J.; Sotomayor, C.; Girault, M.I.; Los Rios Uriarte, M.E.; Sinyavskiy, O.; Aksamit, T.; et al. Digitalization of health care in low- and middle-income countries. Bull. World Health Organ. 2025, 103, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.; Kushniruk, A.; Borycki, E. Barriers to and Facilitators of Artificial Intelligence Adoption in Health Care: Scoping Review. JMIR Hum. Factors 2024, 11, e48633. [Google Scholar] [CrossRef] [PubMed]
- Karami, M.; Madlool, H. Artificial intelligence and digital health in the health systems of developing countries: The challenges and vision of integration in the primary health care setting. Front. Digit. Health 2025, 7, 1532361. [Google Scholar] [CrossRef] [PubMed]
- Borges do Nascimento, I.J.; Abdulazeem, H.; Vasanthan, L.T.; Martinez, E.Z.; Zucoloto, M.L.; Ostengaard, L.; Azzopardi-Muscat, N.; Zapata, T.; Novillo-Ortiz, D. Barriers and facilitators to utilizing digital health technologies by healthcare professionals. npj Digit. Med. 2023, 6, 161. [Google Scholar] [CrossRef] [PubMed]
- Manteghinejad, A.; Javanmard, S.H. Challenges and opportunities of digital health in a post-COVID19 world. J. Res. Med. Sci. 2021, 26, 11. [Google Scholar] [CrossRef] [PubMed]
- Holeman, I.; Cookson, T.P.; Pagliari, C. Digital technology for health sector governance in low and middle income countries: A scoping review. J. Glob. Health 2016, 6, 020408. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ethics and Governance of Artificial Intelligence for Health: WHO Guidance; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Panch, T.; Mattie, H.; Atun, R. Artificial intelligence and algorithmic bias: Implications for health systems. J. Glob. Health 2019, 9, 010318. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. UNICEF’S Digital Health & Information System Annual Report; UNICEF: Hong Kong, China, 2024. [Google Scholar]
- Bank, T.W. Blended Finance. Available online: https://ppp.worldbank.org/blended-finance (accessed on 9 June 2026).
- Owen, A.; Fourie, C.; Ekbladh, L.; Rathod, V. Shaping the Market for Digital Health Tools. A Roadmap to a Sustainable Global Goods Ecosystem; Program for Appropriate Technology in Health (PATH): Seattle, WA, USA, 2025. [Google Scholar]
- Aisyah, D.N.; Lokopessy, A.F.; Naman, M.; Diva, H.; Manikam, L.; Adisasmito, W.; Kozlakidis, Z. The use of digital technology for COVID-19 detection and response management in Indonesia: Mixed methods study. Interact. J. Med. Res. 2023, 12, e41308. [Google Scholar] [CrossRef]
- We need a genomics-savvy healthcare workforce. Nat. Med. 2025, 29, 1877–1878. [CrossRef] [PubMed]
- Jongeneel, C.V.; Kotze, M.J.; Bhaw-Luximon, A.; Fadlelmola, F.M.; Fakim, Y.J.; Hamdi, Y.; Kassim, S.K.; Kumuthini, J.; Nembaware, V.; Radouani, F.; et al. A View on Genomic Medicine Activities in Africa: Implications for Policy. Front. Genet. 2022, 13, 769919. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Publishes New Global Analysis Revealing Major Equity Gaps in Human Genomics Research; WHO: Geneva, Switzerland, 2025. [Google Scholar]
- Tawfik, S.M.; Elhosseiny, A.A.; Galal, A.A.; William, M.B.; Qansuwa, E.; Elbaz, R.M.; Salama, M. Health inequity in genomic personalized medicine in underrepresented populations: A look at the current evidence. Funct. Integr. Genom. 2023, 23, 54. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Carlson, R.; Cawley, M.; Yuan, Q.; Fleming, V.; Yu, F. The Gap Between Technology and Ethics, Especially in Low- and Middle- Income Country Health Information Systems: A Bibliometric Study. In MEDINFO 2021: One World, One Health—Global Partnership for Digital Innovation; SAGE Publications: London, UK, 2022. [Google Scholar]
- El-Saleh, A.A.; Sheikh, A.M.; Albreem, M.A.M. The Internet of Medical Things (IoMT): Opportunities and challenges. Wirel. Netw. 2025, 31, 327–344. [Google Scholar]
- Kadam, D.; Budaragade, A.P.; Salunkhe, U.; Gurav, U.P.; Patil, A. Internet of Medical Things: Architecture, Trends, Challenges, and the Evolution Towards IoMT 5.0. Comput. Netw. Commun. 2025, 3, 148–163. [Google Scholar] [CrossRef]
- Robbiati, C.; Tosti, M.E.; Mezzabotta, G.; Dal Maso, F.; Lulua Sachicola, O.M.; Siene Tienabe, P.; Nsuka, J.; Simonelli, M.; Dente, M.G.; Putoto, G. Improving TB Surveillance and Patients’ Quality of Care Through Improved Data Collection in Angola: Development of an Electronic Medical Record System in Two Health Facilities of Luanda. Front. Public Health 2022, 10, 745928. [Google Scholar] [CrossRef] [PubMed]
- Vota, W. Rwanda Digital Health Revolution is Transforming Healthcare Through Technology; ICTworks: Cape Town, South Africa, 2024. [Google Scholar]
- Kozlakidis, Z.; Kealy, J.; Henderson, M.K. Digitization of Healthcare in LMICs: Challenges and Opportunities in Data Governance and Data Infrastructure. In Digitalization of Medicine in Low- and Middle-Income Countries; Sustainable Development Goals Series; Kozlakidis, Z., Muradyan, A., Sargsyan, K., Eds.; Springer: Cham, Switzerland, 2024. [Google Scholar]
- WHO. Global Initiative on Digital Health. Coordinated Support for Country-Led Digital Health Transformation; WHO: Geneva, Switzerland, 2024. [Google Scholar]
© 2026 by the TIJFS. This is an open-access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).