
Int. J. Front. Sci. , 8(1), 3; doi:10.37978/tijfs.v08i01.003
Case Report
Early Mitral Valve Replacement in Infective Endocarditis Complicated by Ischemic Stroke with Hemorrhagic Transformation: A Case Report
1
Department of Cardiovascular Surgery, Republican Diagnostic Center, Baku AZ1000, Azerbaijan
2
Department of Cardiac Intensive Care, Republican Diagnostic Center, Baku AZ1000, Azerbaijan
*
Correspondence: ziyasahaliyev@gmail.com (Z.S.); anaremrah@gmail.com (A.A.)
Academic Editor:
Muhammad Shoaib Akhtar
How to cite: Shahaliyev, Z.; Amrah, A.; Babayev, H.; Mammadov, V. Early Mitral Valve Replacement in Infective Endocarditis Complicated by Ischemic Stroke with Hemorrhagic Transformation: A Case Report. TIJFS 2026, 8 (1), 3. DOI: 10.37978/tijfs.v08i01.003.
Received: 31 January 2026 / Accepted: 29 June 2026 / Published: 3 July 2026
Abstract
:Background: Infective endocarditis (IE) is a life-threatening condition associated with high morbidity and mortality, particularly when complicated by neurological events. Ischemic stroke occurs in up to 30% of IE cases and poses a major challenge regarding the timing of cardiac surgery due to the risk of hemorrhagic transformation. Case Presentation: We present the case of a 31-year-old Caucasian non-working female featuring progressive dyspnea, orthopnea, palpitations and retrosternal chest discomfort for the last two months. She had no cardiovascular or chronic medical disease before admission. One month prior, she developed sudden right-sided hemiparesis. Neuroimaging showed ischemic stroke with hemorrhagic transformation. Blood cultures grew Streptococcus viridans and transthoracic echocardiography showed a large, mobile vegetation (app. 13 mm) on the mitral valve. Due to high embolic risk, surgical treatment was undertaken following multidisciplinary decision with consideration by cardiology, neurology, neurosurgery, and cardiac surgery teams. After stabilization the patient required urgent mitral valve replacement with a mechanical prosthesis. Postoperatively, the patient was neurologically and hemodynamically intact, with no progression of hemorrhagic transformation. She received a 6-week course of targeted intravenous antibiotic therapy. At 3-month follow-up, she noted marked neurological recovery with motor strength up to approximately 4 out of 5 with independent ambulation and no cardiac complications. Conclusions: This case study suggests that early surgical management is safely available for several patients with ischemic and hemorrhagic transformation complications of IE only when considering carefully tailored patient multidisciplinary evaluation and close perioperative monitoring.
Keywords:
infective endocarditis; ischemic stroke; mitral valve replacement; septic embolism; Streptococcus viridans1. Introduction
Infective endocarditis (IE) is a microbial infection that occurs in the endocardium and usually involves the heart valves. The incidence is estimated between 3 and 9 per 100,000 people per year and in-hospital mortality ranges up to 25%, with improved treatments only helping so much [1]. Neurological complications, including embolic stroke, occur in about 15–30% of IE cases and are associated with poor prognosis [2]. Mitral valve vegetations are a major cause of emboli due to high-pressure left-sided circulation [3].
The decision for performing surgery in stroke patients still under the possibility of hemorrhagic transformation, however, is controversial. This is especially significant with hemorrhagic transformation as it has been noted that this increases the risk of perioperative intracranial bleeding, and complicates the management of anticoagulation. Early surgical intervention is usually suggested in patients with the presence of stubborn embolism and mobile vegetations, according to European Society of Cardiology (ESC) guidelines [4].
This case study is intended to represent decisional aspects of early cardiac surgery in the context of IE, complicated by ischemic stroke and hemorrhagic transformation, and the timing of such surgery, where the optimal clinical time-point remains contentious.
2. Case Presentation
A 31-year-old female presented with complaints of shortness of breath (orthopnea), palpitations, and burning chest pain, behind the sternum. The patient was Caucasian and had no history of employment. She resided independently with no exposure to infectious risks at work. The patient had no previous past medical history and no known chronic diseases such as valvular or congenital heart disease, nor prior hospitalizations. She was not being treated with any medications prior to presentation. She had no known family history of cardiovascular disease, stroke or any of the known genetic disorders. She denied history of intravenous drug use, smoking, alcohol consumption or illicit substance use. Psychosocial history was unremarkable, and no psychosocial stressors or psychiatric conditions were reported. A novel dental work-up without antibiotic prophylaxis was diagnosed as a potential predisposing factor to IE. It was noted that these symptoms were for approximately 2 months before admission to the hospital (Table 1). She also reported general fatigue and malaise, which progressively worsened.

Table 1.
Timeline of clinical events.
| Timeline | Clinical Event |
|---|---|
| 2 months before admission | Onset of progressive dyspnea, orthopnea, fatigue, and palpitations |
| 1 month before admission | Sudden-onset right-sided hemiparesis; hospitalization at another center |
| Initial hospitalization | Diagnosis of ischemic stroke; blood cultures positive for Streptococcus viridans |
| Admission to our center | Detection of large mobile mitral valve vegetation on echocardiography |
| Preoperative period | Cranial CT showing ischemic infarcts with hemorrhagic transformation |
| Multidisciplinary review | Decision for early surgery due to high embolic risk |
| Surgery | Mitral valve replacement with 27 mm mechanical prosthesis |
| Postoperative period | Stable neurological and cardiac status |
| 3-month follow-up | Significant neurological recovery; good prosthetic valve function |
About one month prior to admittance to our clinic, the patient presented with a sudden neurological deficit, characterized by right-sided hemiparesis, causing suspicion for a cerebrovascular event. At first, the patient presented to a medical center and was admitted for two weeks, was initially treated with medical management and then referred to our institution for evaluation and treatment upon symptom onset.
It was observed that a history of dental treatment was noted as a precipitating factor of IE. She had no known history of valvular heart disease. The patient had had a dentist’s office appointment about 1 month before admission to the clinical setting. No peripheral stigmata were described for IE.
Physical examination revealed a holosystolic murmur at the apex of the cardiac cycle. In neurological examination, the right side was hemiparetic and there were no signs of heart failure. Before surgery, the non-contrast cranial CT revealed structures where a hemorrhage process had taken place. Diagnostics on transthoracic echocardiography showed quite a few movable vegetations in the mitral valve (Figure 1). Differential diagnoses included cardioembolic stroke from non-infectious causes; positive blood cultures and echocardiographic findings confirmed IE. Intravenous targeted antibiotic therapy (moxifloxacin and linezolid) was given according to sensitivity testing and continued postoperatively for 6 weeks (Table 2). Considering the patient’s embolic history (ischemic stroke) and the large vegetations, premature surgical intervention was recommended. However, the recent cerebral event resulted in a neurosurgical consultation to determine the incidence of hemorrhagic transformation or surgical contraindications. A non-contrast cranial computed tomography (CT) preoperative scan showed subacute ischemic infarcts with hemorrhagic transformation. The mass effect and midline shift were not significant. Most notably, infarcts were confined to the right parietotemporal and the left frontoparietal lobes (Figure 2). These results were in agreement with embolic stroke from IE. Although there was a hemorrhagic component, infarcts were considered stable and there was no evidence for worsening neurologic function.
Figure 1.
Preoperative transthoracic echocardiography (TTE) revealed a large, mobile vegetation (app. 13 mm) attached to the mitral valve, as indicated by the red arrow.
Figure 1.
Preoperative transthoracic echocardiography (TTE) revealed a large, mobile vegetation (app. 13 mm) attached to the mitral valve, as indicated by the red arrow.
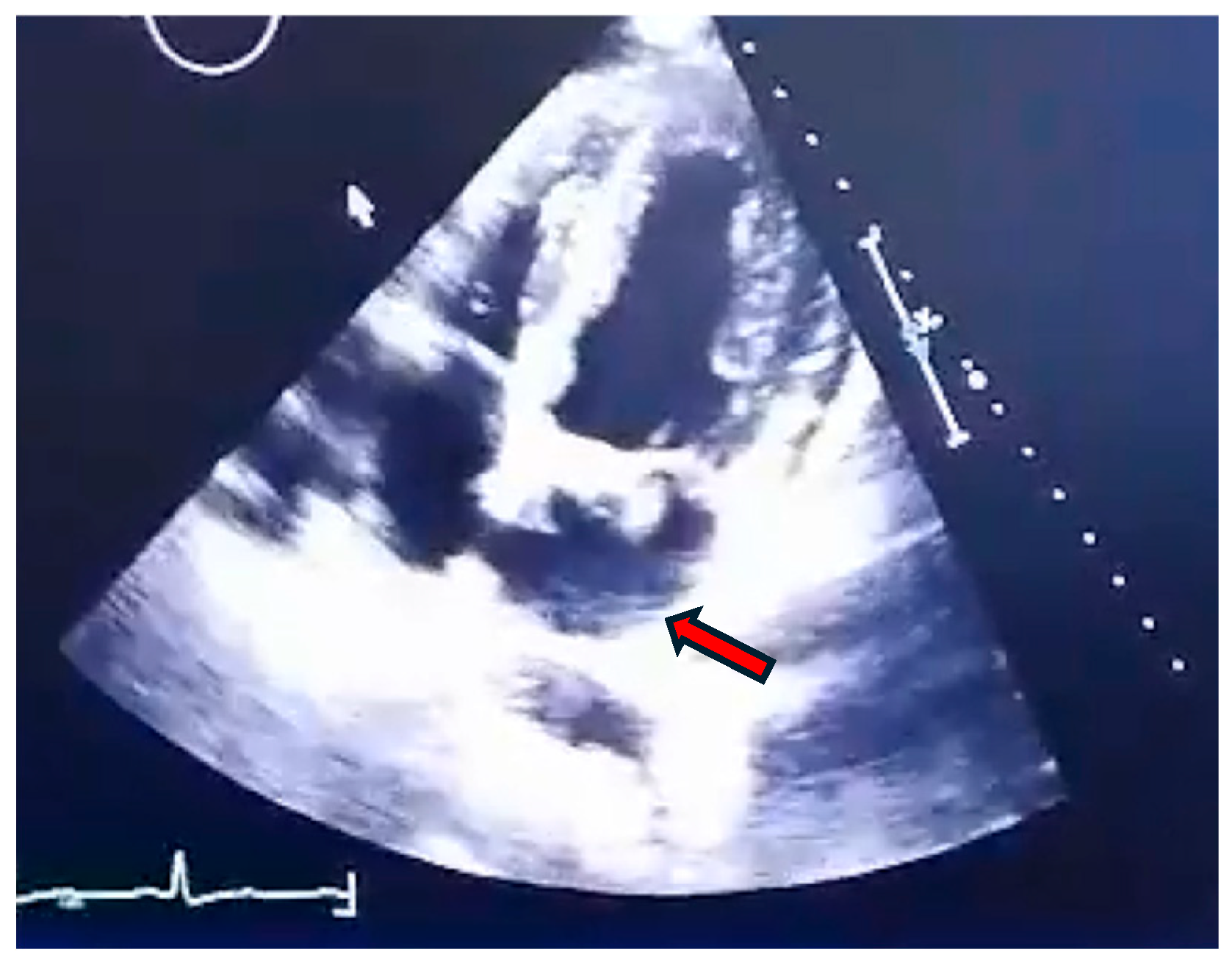
Figure 2.
The preoperative non-contrast cranial CT scan demonstrated infarcted regions (A) with evidence of hemorrhagic transformation (B).
Figure 2.
The preoperative non-contrast cranial CT scan demonstrated infarcted regions (A) with evidence of hemorrhagic transformation (B).
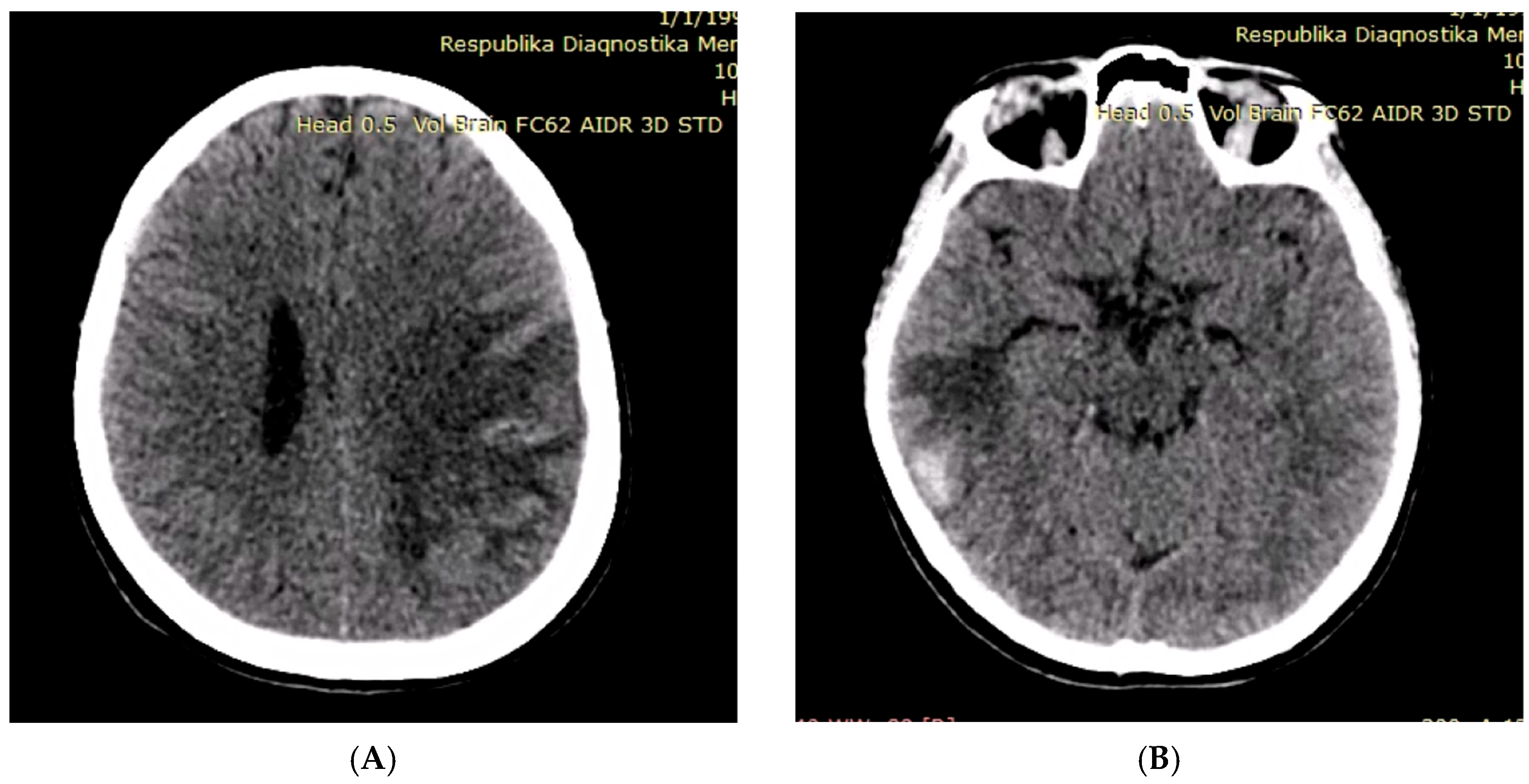
Table 2.
Antimicrobial susceptibility profile of Streptococcus viridans.
| Antibiotic | MIC (µg/mL) | Interpretation |
|---|---|---|
| Ampicillin | 0.12 | Susceptible |
| Vancomycin | 0.5 | Susceptible |
| Gentamicin (high-level) | ≤500 | No high-level resistance |
| Moxifloxacin | 0.25 | Susceptible |
| Linezolid | 1.0 | Susceptible |
| Erythromycin | 2.0 | Resistant |
| Clindamycin | 1.0 | Intermediate |
Interdisciplinary consultation resulted in the decision to perform a surgical intervention due to large (>10 mm), mobile vegetations and a prior embolic event.
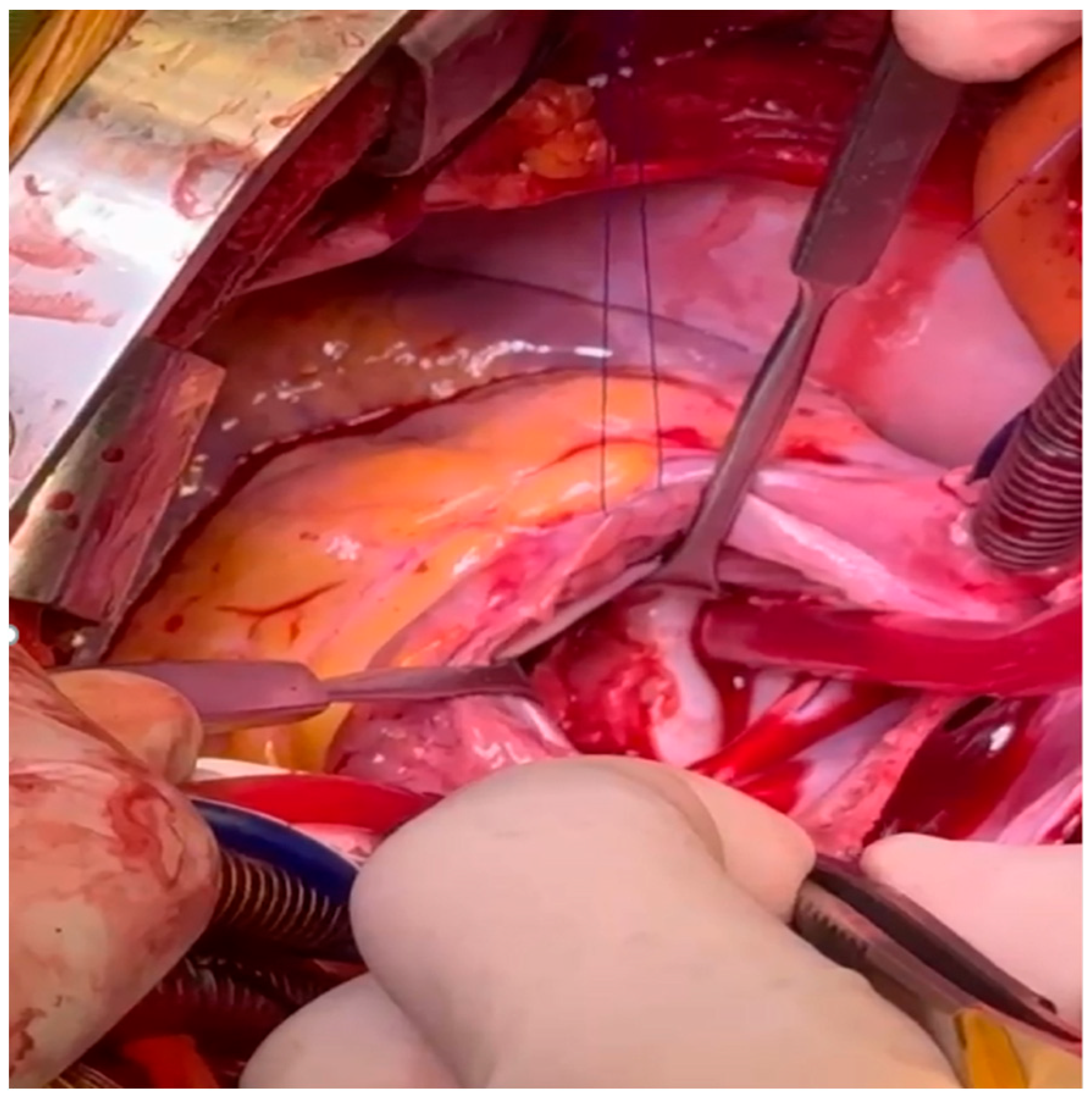
After full preoperative evaluations, the patient underwent cardiac surgery (Figure 3). An intraoperative image of a destroyed native mitral valve, with vegetative material in it, was visualized. Mitral valve replacement was performed using a 27 mm St. Jude mechanical prosthesis by surgeons. A mechanical prosthesis was chosen because of the patient’s young age and the need for permanent durability. The topic of lifelong anticoagulation, including discussions regarding future pregnancy, was discussed with the patient. This infected and weakened mitral annulus was repaired with a bovine pericardial patch.
Figure 3.
Intraoperative image showing the native mitral valve with large vegetations and extensive damage to the endocardial surface of the mitral annulus.
Figure 3.
Intraoperative image showing the native mitral valve with large vegetations and extensive damage to the endocardial surface of the mitral annulus.
The postoperative period was uneventful with respect to cardiac and neurological status. The patient remained hemodynamically stable, and no progression of her neurologic symptoms or new hemorrhagic complications were observed. Postoperative transthoracic echocardiography confirmed appropriate prosthetic valve function without paravalvular leak or obstruction.
The patient continued intravenous antibiotic therapy postoperatively according to IE guidelines and was followed closely by the multidisciplinary team. Plans were made for extended neurological rehabilitation and outpatient cardiology follow-up. At 3-month follow-up, the patient demonstrated marked neurological recovery with improved motor strength and remained asymptomatic from a cardiac standpoint.
3. Discussion
IE poses serious complications when associated with neurological events. The risk of embolization is increased in the presence of large (>10 mm), mobile vegetations, particularly those involving the mitral valve and caused by aggressive organisms such as Streptococcus viridans [5]. Guidelines from the ESC support urgent surgery even after ischemic stroke in the absence of major hemorrhagic risk [3].
Hemorrhagic transformation represents a critical factor influencing surgical timing in IE, as it increases the risk of perioperative intracranial bleeding. In this case, surgery was undertaken after confirming radiological stability and absence of mass effect. Perioperative anticoagulation was carefully managed with close neurological monitoring.
In this case, although imaging showed hemorrhagic transformation, early surgical intervention was performed after careful evaluation. The decision was based on persistent embolic risk, clinical stability, and no progression of neurological symptoms. Studies have shown that timely surgery in select patients with IE and cerebrovascular complications can significantly improve outcomes [2,3].
Several case reports have described complex presentations of IE with embolic complications. Abdi et al. reported IE associated with septic emboli [6], while Dahir et al. highlighted severe mitral regurgitation as a prognostic factor [7]. Other reports have described rare presentations such as post-splenectomy endocarditis [8]. These findings support individualized management strategies in high-risk patients.
The decision to proceed with surgery was based on a multidisciplinary assessment integrating neurological stability, imaging findings, and the high embolic risk associated with large, mobile vegetations. This approach aligns with current guideline recommendations emphasizing individualized decision-making. Close perioperative monitoring and careful anticoagulation management were essential components in minimizing the risk of hemorrhagic progression.
4. Conclusions
This case illustrates that early surgery in patients with IE complicated by ischemic stroke may be beneficial and life-saving. Multidisciplinary decision-making, appropriate imaging, and individualized risk assessment are crucial in optimizing outcomes in such complex cases. Limitations of this study include the single-patient nature of the report and the inability to generalize surgical timing recommendations.
Author Contributions
Conceptualization, A.A. and Z.S.; methodology, A.A.; software, Z.S.; validation, A.A., Z.S., H.B. and V.M.; formal analysis, Z.S.; investigation, A.A. and Z.S.; resources, H.B.; data curation, V.M.; writing—original draft preparation, Z.S.; writing—review and editing, A.A.; visualization, Z.S.; supervision, A.A.; project administration, A.A.; All authors have read and agreed to the published version of the manuscript.
Funding
No external funding was received for this study.
Informed Consent Statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Data Availability Statement
The data supporting the findings of this study are included within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cahill, T.J.; Baddour, L.M.; Habib, G.; Hoen, B.; Salaun, E.; Pettersson, G.B.; Schäfers, H.J.; Prendergast, B.D. Challenges in infective endocarditis. J. Am. Coll. Cardiol. 2017, 69(3), 325–344. [Google Scholar] [CrossRef] [PubMed]
- Thuny, F.; Avierinos, J.F.; Tribouilloy, C.; Giorgi, R.; Casalta, J.P.; Milandre, L.; Brahim, A.; Nadji, G.; Riberi, A.; Collart, F.; et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis. Eur. Heart J. 2007, 28(9), 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the management of infective endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2023, 44(39), 3948–4042. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G., Jr.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications. Circulation 2015, 132(15), 1435–1486. [Google Scholar] [CrossRef] [PubMed]
- Vilacosta, I.; Graupner, C.; San Román, J.A.; Sarriá, C.; Ronderos, R.; Fernández, C.; Mancini, L.; Sanz, O.; Sanmartín, J.; Stoermann, W. Risk of embolization after institution of antibiotic therapy for infective endocarditis. J. Am. Coll. Cardiol. 2002, 39(9), 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Abdi, I.A.; Nur, A.A.; Duale, A. A Case of Infective Endocarditis and Pulmonary Septic Emboli Caused by Coagulase-Negative Staphylococci. Res. Rep. Clin. Cardiol. 2022, 13, 95–99. [Google Scholar] [CrossRef]
- Dahir, O.F.; Hassan, M.O.; Adan, A.S.; Abdi, A.E.; Abdi, I.A. Infective Endocarditis Complicated by Severe Mitral Regurgitation and Markedly Elevated Troponin Levels as A Prognostic Marker: A Case Report. Res. Rep. Clin. Cardiol. 2025, 16, 9–14. [Google Scholar] [CrossRef]
- Abdi, I.A.; Nur, A.A.; Karataş, M.; Mohamud, M.F. Post-splenectomy native valve endocarditis caused by coagulase negative staphylococci: A rare case report. Ann. Med. Surg. 2022, 78. [Google Scholar] [CrossRef] [PubMed]
© 2026 by the TIJFS. This is an open-access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).