
Int. J. Front. Sci. , 8(1), 1; doi:10.37978/tijfs.v08i01.001
Comment
An Overview of Nipah Virus Infection: Epidemiology, Pathogenesis, Diagnostic Challenges, and Global Research Priorities
1
Department of Laboratory Medicine, Sheikh Khalifa Hospital, Fujairah, United Arab Emirates
2
Department of Laboratory Medicine, Fujairah Hospital, Fujairah, United Arab Emirates
*
Correspondence: shafiqahmadchudhary@gmail.com
Academic Editor:
Muhammad Shoaib Akhtar
How to cite: Chudhary, S.A.; Zeb, I.; Khan, D.; Gul, I.; Saeed, M. An Overview of Nipah Virus Infection: Epidemiology, Pathogenesis, Diagnostic Challenges, and Global Research Priorities. TIJFS 2026, 8 (1), 1. DOI: 10.37978/tijfs.v08i01.001.
Received: 1 February 2026 / Accepted: 11 April 2026 / Published: 14 May 2026
Abstract
:Nipah virus (NiV) is a highly pathogenic zoonotic henipavirus that causes severe respiratory and neurological disease with case-fatality rates of 40–75%. Despite its epidemic potential, no licensed vaccines or specific antiviral therapies are currently available. Consequently, the World Health Organization (WHO) has prioritized NiV and established a research and development roadmap to accelerate the development of diagnostics, therapeutics, and vaccines. Since its emergence during outbreaks in Malaysia and Singapore in 1998–1999, NiV has caused recurrent outbreaks in South and Southeast Asia, including multiple events in West Bengal, India, with the most recent cases reported in January 2026. NiV transmission occurs through direct contact with infected animals, consumption of contaminated food products, or human-to-human transmission, with fruit bats (Pteropus spp.) serving as natural reservoirs. Clinical manifestations range from mild illness to severe acute respiratory disease and fatal encephalitis, with rapid neurological deterioration. Laboratory diagnosis relies primarily on molecular detection by RT–PCR and serological assays, such as ELISA. However, diagnostic development is limited by the scarcity of well-characterized clinical specimens, gaps in external quality assessment, and insufficient surveillance data. This article reviews current laboratory diagnostic strategies and outlines WHO research priorities for 2024–2029, emphasizing rapid point-of-care diagnostics, strengthened laboratory capacity, particularly in low- and middle-income countries, and integration within One Health surveillance frameworks to improve outbreak preparedness and response.
Keywords:
laboratory diagnostics; medical countermeasures; Nipah virus; outbreak preparedness; zoonotic infection1. Introduction
NiV is an emerging zoonotic pathogen with significant epidemic potential. NiV infection is associated with severe disease and high mortality, with case-fatality rates ranging from 40% to 75% across reported outbreaks, depending on local capabilities, early detection, and clinical management. Currently, no licensed vaccines or specific antiviral therapies are available for the prevention or treatment of NiV infection [1].
In response to the public health threat posed by NiV and related henipaviruses, the WHO identified NiV as a priority pathogen under its R&D Blueprint and released an advanced draft research and development roadmap in 2019. This roadmap, updated with strategic goals for 2024–2029, aims to accelerate the development of diagnostics, therapeutics, and vaccines to enable rapid and effective outbreak response [1,2].
2. Virology and Genetic Structure
NiV is an enveloped, negative-sense, single-stranded RNA virus that belongs to the family Paramyxoviridae and the genus Henipavirus. The viral genome encodes six major structural proteins: nucleocapsid (N), phosphoprotein (P), matrix (M), fusion (F), attachment glycoprotein (G), and large polymerase (L) protein. The G and F glycoproteins are critical for viral attachment and membrane fusion, mediating entry into host cells [3].
The attachment glycoprotein G binds with high affinity to the cellular ephrin ligands Ephrin-B2 and Ephrin-B3, which serve as the principal functional receptors for NiV in both human and bat hosts [4]. Ephrin-B2 and ephrin-B3 are transmembrane ligands involved in bidirectional signaling with Eph receptor tyrosine kinases and play critical roles in vascular development and neuronal guidance. Structural and biochemical studies have demonstrated that the NiV G glycoprotein adopts a six-bladed β-propeller architecture that engages the G–H loop of ephrin-B2/B3 with high specificity. This interaction mimics the natural binding interface between ephrins and Eph receptors, enabling the virus to exploit a conserved cellular signaling pathway for host cell attachment [5].
Upon receptor engagement, conformational changes in the G glycoprotein are transmitted to the metastable pre-fusion form of the F glycoprotein. The F protein, which is synthesized as an inactive precursor (F0), undergoes proteolytic cleavage by host endosomal proteases, such as Cathepsin L, to generate the fusion-competent subunits F1 and F2. Following receptor-induced triggering, the F protein undergoes a dramatic structural rearrangement from a pre-fusion to a post-fusion conformation, exposing the hydrophobic fusion peptide that inserts into the host cell membrane. This process results in the formation of a six-helix bundle structure that brings the viral envelope and cellular membrane into close proximity, ultimately facilitating membrane merger and the delivery of the viral ribonucleoprotein complex into the host cytoplasm [6].
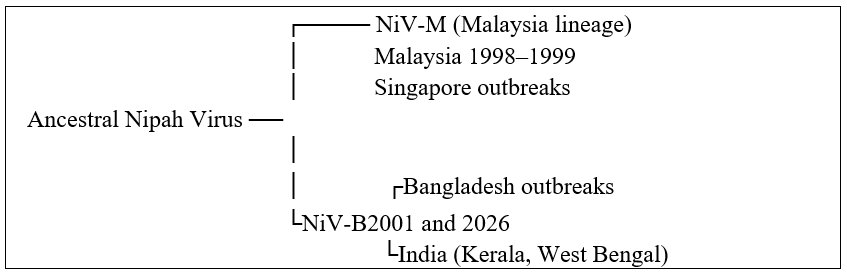
The distribution of ephrin-B2 and ephrin-B3 in host tissues provides a mechanistic explanation for NiV tissue tropism and pathogenesis. Ephrin-B2 is highly expressed in arterial endothelial cells, smooth muscle cells, and various epithelial tissues, whereas Ephrin-B3 is predominantly expressed in neurons within the central nervous system. Consequently, NiV infection is characterized by widespread endothelial involvement, vasculitis, and severe encephalitis. Importantly, these receptors are highly conserved among mammals, including fruit bats of the genus Pteropus, which serve as natural reservoir hosts [7]. The strong structural conservation of ephrin-B2/B3 across species enables efficient cross-species receptor recognition, facilitating zoonotic spillover events. Genetic analyses have identified at least two major NiV lineages: the Malaysia lineage (NiV-M) and the Bangladesh lineage (NiV-B). These lineages differ in geographic distribution, transmission dynamics, and clinical outcomes, with NiV-B being more frequently associated with human-to-human transmission and higher case-fatality rates [8,9]. The phylogenetic relationships are illustrated in Figure 1, and a comparative analysis of both lineages is presented in Table 1.
Figure 1.
Phylogenetic relationship between the Nipah virus lineages.
Genetic diversity among circulating strains has important implications for diagnostic sensitivity, therapeutic efficacy, and vaccine design [4,5,10].

| Parameter | NiV-M (Malaysia Lineage) | NiV-B (Bangladesh Lineage) |
|---|---|---|
| Geographic distribution | Malaysia, Singapore; related bat strains in Thailand/Cambodia | Bangladesh, India |
| Major outbreak period | 1998–1999 outbreak linked to pigs | Recurrent outbreaks since 2001 and 2026 |
| Transmission dynamics | Mainly animal-to-human (pigs acted as amplifying hosts) | Frequent human-to-human transmission |
| Primary spillover route | Pig farming exposure | Contaminated date-palm sap, bats, person-to-person |
| Case fatality rate | ~40% | ~60–75% (often higher) |
| Clinical presentation | Predominantly encephalitis, less respiratory involvement | Severe respiratory disease + encephalitis |
| Incubation period | Generally, longer | Often shorter |
| Viral shedding | Lower respiratory shedding | Higher replication in respiratory tract |
| Genome features | ~18,246 nucleotide genome | ~18,252 nucleotide genome with small sequence differences |
| Genetic difference | Reference lineage | ~9% genomic difference vs. NiV-M |
| Public health pattern | Single large outbreak | Annual or periodic spillover events |
| Phylogenetic clade | Clade II (Malaysia genotype) | Clade I (Bangladesh genotype) |
| Early identification approach | Monitoring individuals with pig exposure presenting with febrile illness or encephalitis | Syndromic surveillance for acute febrile illness, respiratory symptoms, and encephalitis |
| Diagnostic methods | RT-PCR detection of viral RNA and serological testing (IgM/IgG) in exposed individuals | RT-PCR and serological assays combined with active screening of symptomatic contacts |
3. Transmission and Pathogenesis
Fruit bats of the genus Pteropus, commonly referred to as flying foxes, are the natural reservoirs of NiV. Viral maintenance in bat populations enables periodic spillovers into humans and domestic animals. Human infection occurs through direct contact with infected animals, consumption of food contaminated with bat saliva, urine, or excreta, or close contact with infected individuals [10,11].
Human-to-human transmission has been well documented, particularly in healthcare settings and among household contacts. The incubation period typically ranges from 3 to 14 days, although incubation periods of up to 45 days have been reported in rare cases [12].
Following infection, NiV exhibits systemic dissemination with a strong tropism for endothelial and neuronal tissues, leading to widespread vasculitis, encephalitis, and respiratory complications. These pathogenic mechanisms contribute to the rapid clinical deterioration in severe cases [13].
4. Clinical Manifestations
NiV infection presents a wide clinical spectrum, ranging from asymptomatic infection to severe, rapidly progressive disease. Early symptoms are nonspecific and include fever, headache, myalgia, vomiting, and sore throat. As the disease progresses, neurological manifestations such as dizziness, somnolence, altered mental status, and focal or generalized neurological deficits may develop, consistent with acute encephalitis [14].
Severe disease is frequently characterized by seizures and rapid progression to coma within 24–48 h of onset. Respiratory involvement, including atypical pneumonia and acute respiratory distress syndrome (ARDS), has been reported and is more commonly associated with increased transmissibility and poor outcomes [15,16].
5. Global Epidemiology and Recent Outbreaks
NiV was first recognized during outbreaks of respiratory illness in swine and encephalitis in humans in Malaysia between 1998 and 1999, followed by cases in Singapore in 1999 linked to pig exposure [17,18]. Since then, recurrent outbreaks and sporadic cases have been reported in South and Southeast Asia, particularly in Bangladesh and India.
A recent (NiV) infection in India resulted in the death of a 25-year-old nurse in West Bengal in early 2026 due to post-infectious complications. As of January 26, 2026, two laboratory-confirmed NiV cases from West Bengal State were reported to the World Health Organization [4,5]. This episode constitutes the third documented NiV outbreak in West Bengal, following prior outbreaks in (2001) and (2007) [5,10,11]. NiV is a highly pathogenic zoonotic paramyxovirus associated with a case-fatality rate ranging from 40% to 75%, depending on the outbreak context and healthcare capacity. The recurrence of outbreaks in this region underscores the persistent risk of NiV re-emergence and highlights the critical need for sustained epidemiological surveillance, rapid diagnostic capacity, and strengthened outbreak preparedness and response systems.
6. Current Treatment and Preventive Options
Currently, no licensed vaccines or specific antiviral therapies are available for NiV infection. Clinical management is limited to supportive care, including management of respiratory failure, seizures, and cerebral edema, alongside strict infection prevention and control practices [11].
Multiple vaccine and therapeutic candidates are in various stages of preclinical and clinical development worldwide. These efforts are guided by the WHO R&D roadmap, which prioritizes interventions with the potential for rapid deployment during outbreaks [1].
7. Diagnostic Approaches and Challenges
Laboratory confirmation of NiV infection can be achieved during both acute and convalescent phases using a combination of diagnostic assays [7], a summary of laboratory diagnostic approaches at both phases is shown in Table 2. Molecular detection of viral RNA by reverse transcription polymerase chain reaction (RT-PCR) remains the gold standard during the acute phase, providing high sensitivity and specificity. RT-PCR typically targets conserved viral genomic regions, such as the nucleocapsid (N), phosphoprotein (P), and fusion (F) genes. Serological assays, including enzyme-linked immunosorbent assays (ELISA) for NiV-specific IgM and IgG antibodies, are essential for retrospective diagnosis and sero-epidemiological studies [21]. The kinetics of antibody responses are clinically informative: IgM antibodies typically appear within 3–10 days post-infection, serving as markers of recent or ongoing infection, whereas IgG antibodies emerge later and persist, indicating past exposure and potential immunity. Rapid diagnostic tests (RDTs) and syndromic multiplex panels are increasingly recognized as critical tools for point-of-care testing, especially in outbreak scenarios and low-resource settings [21]. The incorporation of both molecular and serological testing enhances diagnostic accuracy and informs clinical and public health decision-making.
Table 2.
Diagnostic approaches.
| Phase Day Post-Infection | Diagnostic Test | Marker Detection | Clinical/Epidemiological Relevance | Reference |
|---|---|---|---|---|
| Acute Phase | RT–PCR | Viral RNA | Gold standard for early diagnosis; high sensitivity and specificity | [21] |
| (Day 0–10) | ||||
| Early Seroconversion (Day 3–10) | ELISA/Serology | IgM antibodies | Indicates recent or ongoing infection; useful for early clinical decisions | [22] |
| Convalescent/Later Phase (Day 10+) | ELISA/Serology | IgG antibodies | Indicates past exposure; useful for sero-epidemiological studies and immunity assessment | [22] |
| Beyond Day 14 | Serology/ELISA | IgG antibodies persist | Indicates past exposure | [22] |
8. Reliability and Validation Limitations
The validation of diagnostic assays for NiV has been constrained by the limited availability of well-characterized human clinical specimens. Consequently, animal-derived samples are frequently used for assay evaluations. For example, serum or tissue samples from experimentally infected Syrian hamsters (Mesocricetus auratus) are widely used because this model closely reproduces the pathological and virological features of human NiV infection, including respiratory disease and encephalitis. Viral replication patterns and antigen expression in hamsters are comparable to those observed in human infection, making these samples suitable for preliminary diagnostic assay validation [21,22].
Persistent gaps include limited routine external quality assessments, incomplete characterization of viral and antibody kinetics, outdated proficiency testing panels, and insufficient surveillance data, as highlighted in successive WHO assessments [23].
9. Research Priorities and Strategic Recommendations
In response to these challenges, a consensus group of 15 subject matter experts has outlined strategic priorities for 2024–2029 to strengthen global preparedness for NiV and related henipavirus outbreaks. Key recommendations include: (1) Development and deployment of affordable, easy-to-use point-of-care diagnostic tests capable of detecting all known NiV lineages. (2) Expansion of access to well-characterized clinical specimens to support diagnostic validation and regulatory approvals. (3) Updating target product profiles to align with current epidemiology and leverage advances in multiplex diagnostic technologies. (4) Strengthening local laboratory capacity and integrating diagnostics into One Health surveillance frameworks. (5) Accelerating the development of effective therapeutics and vaccines with clear pathways for emergency use during outbreaks [1].
Despite advances in diagnostics, a critical knowledge gap in NiV research lies in defining the host molecular pathways modulated during infection. Understanding the host–pathogen biology of NiV and potently suppressing innate immunity, particularly interferon signaling, through phosphoprotein-mediated inhibition of antiviral signaling, yet the broader network of dysregulated pathways, including NF-κB signaling, endothelial injury, and neuroinflammation, remains poorly defined. Integrative multi-omics profiling of infected tissues and survivor cohorts could identify biomarkers of disease severity and uncover host pathways exploitable for therapeutic intervention. Targeting conserved host responses rather than viral proteins may offer more durable antiviral strategies [23]. Addressing these questions will require coordinated global research efforts, particularly strengthened research capacity, and longitudinal studies in outbreak-prone low- and middle-income regions.
10. Conclusions
NiV continues to represent a substantial global public health threat due to its high case-fatality rate, potential for epidemic spread, and the absence of licensed vaccines or targeted antiviral therapies. Despite advances in understanding its virology, transmission dynamics, and clinical spectrum, significant gaps remain in diagnostic preparedness, surveillance coverage, and access to well-validated diagnostic tools, particularly in low- and middle-income countries. Strengthening diagnostic capacity through the development and deployment of sensitive, lineage-inclusive, and field-deployable assays, alongside improved quality assurance and surveillance systems, is essential for timely outbreak detection and response. Coordinated international efforts aligned with WHO research and development priorities are critical for accelerating the availability of effective diagnostics and medical countermeasures and enhancing global readiness for future NiV outbreaks.
Author Contributions
S.A.C.: Conceptualization, manuscript writing, and final draft review. I.Z., D.K., I.G., M.S.: Literature review and critical revision of the manuscript, and approval of the final draft. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
No subject involved in this study.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
We would like to acknowledge the valuable contributions of researchers and laboratory professionals who work tirelessly to ensure timely and accurate diagnosis of life threating disease conditions.
Conflicts of Interest
None.
References
- Moore, K.A.; Mehr, A.J.; Ostrowsky, J.T.; Ulrich, A.K.; Moua, N.M.; Fay, P.C.; Hart, P.J.; Golding, J.P.; Benassi, V.; Preziosi, M.P.; et al. Measures to prevent and treat Nipah virus disease: Research priorities for 2024–29. Lancet Infect. Dis. 2024, 24, e707–e717. [Google Scholar] [CrossRef] [PubMed]
- Higgs, E.S. 14 Accelerating Development of Therapeutics for Preparedness, Response, and a More Secure World. In Principles and Practice of Emergency Research Response; Springer International Publishing: Cham, Switzerland, 2024; pp. 315–343. [Google Scholar]
- Madhukalya, R.; Yadav, U.; Parray, H.A.; Raj, N.; Lupitha, S.S.; Kumar, V.; Saroj, A.; Agarwal, V.; Kumar, D.; Das, S.; et al. Nipah virus: Pathogenesis, genome, diagnosis, and treatment. Appl. Microbiol. Biotechnol. 2025, 109, 158. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Yan, S.; Wang, N.; He, W.; Guan, H.; He, C.; Wang, Z.; Lu, M.; He, W.; Ye, R.; et al. Emergence and adaptive evolution of Nipah virus. Transbound. Emerg. Dis. 2020, 67, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Pernet, O.; Wang, Y.E.; Lee, B. Henipavirus receptor usage and tropism. Henipaviru Ecol. Mol. Virol. Pathog. 2012, 359, 59–78. [Google Scholar]
- White, J.M.; Delos, S.E.; Brecher, M.; Schornberg, K. Structures and mechanisms of viral membrane fusion proteins: Multiple variations on a common theme. Crit. Rev. Biochem. Mol. Biol. 2008, 43, 189–219. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Broder, C.C.; Nikolov, D.B. Ephrin-B2 and ephrin-B3 as functional henipavirus receptors. Semin. Cell Dev. Biol. 2012, 23, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Satapathy, T.; Sahu, P.; Satapathy, A.; Bhardwaj, S.K.; Satapathy, A.; Yadav, N.; Chandrakar, K.; Chandrakar, M. Nipah Virus (NiV) at the Human-Animal-Environment Interface: Emerging Insights into Spillover Dynamics, Neurotropism, and Future Pandemic Risk. J. Drug Deliv. Ther. 2025, 15, 124–133. [Google Scholar] [CrossRef]
- Laing, E.D.; Navaratnarajah, C.K.; Da Silva, S.C.; Petzing, S.R.; Xu, Y.; Sterling, S.L.; Marsh, G.A.; Wang, L.-F.; Amaya, M.; Nikolov, D.B.; et al. Structural and functional analyses reveal promiscuous and species specific use of ephrin receptors by Cedar virus. Proc. Natl. Acad. Sci. USA 2019, 116, 20707–20715. [Google Scholar] [CrossRef] [PubMed]
- De Campos, G.M.; Cella, E.; Kashima, S.; Alcântara, L.C.J.; Sampaio, S.C.; Elias, M.C.; Giovanetti, M.; Slavov, S.N. Updated insights into the phylogenetics, phylodynamics, and genetic diversity of Nipah virus (NiV). Viruses 2024, 16, 171. [Google Scholar] [CrossRef] [PubMed]
- Mire, C.E.; Satterfield, B.A.; Geisbert, J.B.; Agans, K.N.; Borisevich, V.; Yan, L.; Chan, Y.-P.; Cross, R.W.; Fenton, K.A.; Broder, C.C.; et al. Pathogenic differences between Nipah virus Bangladesh and Malaysia strains in primates: Implications for antibody therapy. Sci. Rep. 2016, 6, 30916. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Nipah Virus Infection—India (Disease Outbreak News: DON593). Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON593 (accessed on 30 January 2026).
- Branda, F.; Ceccarelli, G.; Giovanetti, M.; Albanese, M.; Binetti, E.; Ciccozzi, M.; Scarpa, F. Nipah virus: A zoonotic threat Re-Emerging in the wake of global public health challenges. Microorganisms 2025, 13, 124. [Google Scholar] [CrossRef] [PubMed]
- Mougari, S.; Gonzalez, C.; Reynard, O.; Horvat, B. Fruit bats as natural reservoir of highly pathogenic henipaviruses: Balance between antiviral defense and viral tolerance. Curr. Opin. Virol. 2022, 54, 101228. [Google Scholar] [CrossRef] [PubMed]
- Burroughs, A.L.; Durr, P.A.; Boyd, V.; Graham, K.; White, J.R.; Todd, S.; Barr, J.; Smith, I.; Baverstock, G.; Meers, J.; et al. Hendra virus infection dynamics in the grey-headed flying fox (Pteropus poliocephalus) at the southern-most extent of its range: Further evidence this species does not readily transmit the virus to horses. PLoS ONE 2016, 11, e0155252. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Nipah Virus. 26 January 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/nipah-virus (accessed on 26 January 2026).
- Liew, Y.J.M.; Ibrahim, P.A.S.; Ong, H.M.; Chong, C.N.; Tan, C.T.; Schee, J.P.; Román, R.G.; Cherian, N.G.; Wong, W.F.; Chang, L.-Y. The immunobiology of Nipah virus. Microorganisms 2022, 10, 1162. [Google Scholar] [CrossRef] [PubMed]
- Levine, C.B.; Sauer, L.M.; McLellan, S.L.; Evans, J.D. State of the Science Working Group of the National Ebola Training and Education Center’s (NETEC’s) Special Pathogens Research Network (SPRN) Blanton Lucas Chan Justin Davey Rick Frank Maria Gaby Hynes Noreen Shenoy Erica. Nipah virus: A summary for clinicians. Int. J. Emerg. Med. 2025, 18, 126. [Google Scholar] [PubMed]
- Racca, F.; Vianello, A.; Mongini, T.; Ruggeri, P.; Versaci, A.; Vita, G.L.; Vita, G. Practical approach to respiratory emergencies in neurological diseases. Neurol. Sci. 2020, 41, 497–508. [Google Scholar] [CrossRef] [PubMed]
- Ralph, R.; Lew, J.; Zeng, T.; Francis, M.; Xue, B.; Roux, M.; Ostadgavahi, A.T.; Rubino, S.; Dawe, N.J.; Al-Ahdal, M.N.; et al. 2019-nCoV (Wuhan virus), a novel Coronavirus: human-to-human transmission, travel-related cases, and vaccine readiness. J. Infect. Dev. Ctries. 2020, 14(01), 3–17. [Google Scholar] [CrossRef]
- Daniels, P.; Ksiazek, T.; Eaton, B.T. Laboratory diagnosis of Nipahand Hendra virus infections. Microbes Infect. 2001, 3(4), 289–295. [Google Scholar] [CrossRef]
- Garbuglia, A.R.; Lapa, D.; Pauciullo, S.; Raoul, H.; Pannetier, D. Nipah virus: An overview of the current status of diagnostics and their role in preparedness in endemic countries. Viruses 2023, 15, 2062. [Google Scholar] [CrossRef] [PubMed]
- Hantabal, J.; Salguero, F.J.; Carroll, M.W. Current knowledge on the host-pathogen interactions of henipaviruses and novel platforms to enable further characterisation. eBioMedicine 2026, 123, 106110. [Google Scholar] [CrossRef] [PubMed]
© 2026 by the TIJFS. This is an open-access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).